 KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Volume 38(4); 2023 > Article
-
Review article
Prevention of myopia progression using orthokeratology -
Stephanie Suzanne S. Garcia1,2
 , Changzoo Kim1,2,3
, Changzoo Kim1,2,3 -
Kosin Medical Journal 2023;38(4):231-240.
DOI: https://doi.org/10.7180/kmj.23.141
Published online: December 26, 2023
1Department of Ophthalmology, University of California, Los Angeles, Los Angeles, CA, USA
2Stein Eye Institute, University of California, Los Angeles, Los Angeles, CA, USA
3Department of Ophthalmology, Kosin University College of Medicine, Busan, Korea
- Corresponding Author: Changzoo Kim, MD, PhD Department of Ophthalmology, Kosin University College of Medicine, 262 Gamcheon-ro, Seo-gu, Busan 49267, Korea Tel: +82-51-990-6857 Fax: +82-51-990-6857 E-mail: changzoo@hanmail.net
Copyright © 2023 Kosin University College of Medicine.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 665 Views
- 23 Download
Abstract
- The prevalence of myopia in children and juveniles has increased significantly in Korea and worldwide; in particular, the rates of myopia and high myopia in East Asia have grown rapidly. Myopia is easily corrected with spectacles or contact lenses. However, as children grow and mature, myopia can progress irreversibly and lead to vision-threatening complications. Thus, the prevention of myopia progression is an essential treatment goal. Many treatment strategies are being employed, including atropine eyedrops, specialized glasses, and orthokeratology (Ortho-K) lenses. Ortho-K is an effective treatment in managing myopia progression by lowering the rate of increase in refractive error and axial length. In this article, we review Ortho-K as a treatment for myopia progression, its history, mechanism, treatment regimen, and safety profile.
- Myopia, more commonly known as nearsightedness, is a condition in which the image of a distant object is formed in front of the retina due to a mismatch between the optical refractive power of the eye and the axial length. Myopia is derived from the Greek myōps (myein, to close + ōps, the eye) meaning “short-sighted.” This concept dates back to B.C. 350 where a link between myopia, bulging eyes, frequent blinking, eyelid squeezing, close reading were theorized [1,2]. Now, after two millennia, myopia is one of the most common eye conditions worldwide. This increased prevalence has led to increased interest and awareness of myopia progression and the risk of sight-threatening complications. To mitigate the risk of these complications, many strategies to delay the progression of myopia are being used and investigated. Through this review based on traditional methods [3], we focused on the role of orthokeratology (Ortho-K) in decreasing the progression of myopia.
Introduction
- Myopia is prevalent worldwide but has a strikingly higher prevalence in East Asia [4]. The prevalence in schoolchildren were reported at 80.2% in Korea [5], 80.7% in China [6], 76.67% in Taiwan [4], and 74.2% in Singapore [7]. In addition, an increased prevalence was also found in children of Asian descent living elsewhere [8]. With these numbers projected to rise in the coming decades, myopia is considered a global epidemic and an imminent public health concern. The estimated worldwide prevalence of myopia was 22.9% of the world population [9]. It is projected that by 2050, 49.8% of the population will be myopic, with 9.8% having high myopia of more than 5.00 D [9]. Traditionally, vision is improved in myopes by glasses, contact lenses, or refractive surgery. However, progression to high and pathologic myopia can lead to an array of complications including myopic maculopathy, retinal tears and detachments which causes concern for low vision and blindness [10].
Epidemiology of myopia
- Generally, children are born with hyperopic eyes. Emmetropization of eyes occur within first 2 years after birth [11]. Significant changes in the axial length, cornea, and crystalline lens contribute to emmetropization in the early years of life and are usually completed at age 6 years [12]. Factors which interfere with this process and disrupt the balance of anatomical development have been known to cause myopia in both animal and human models [13,14]. Although the exact mechanism is unknown, the occurrence and progression of myopia is determined by a complex interplay of environmental and genetic factors. Environmental factors such as intensive education at a young age are contributory to increased myopia while others, such as increased time doing outdoor activities in bright light have been identified to have a protective effect [15-17]. In 2018, the Ministry of Education in China released a Comprehensive Plan to Prevent Nearsightedness among Children and Teenagers (CPPNCT) to curb myopia among children [18]. In 2023, these guidelines were updated and included reducing electronic device use, adequate lighting in schools, and at least 2 hours of outdoor activities daily [19]. Although the recent increase in myopia has been largely due to environmental changes, genetic factors have been postulated for many years as evidenced by family clustering and twin studies [7,14]. Studies of genetic linkage have identified almost 200 genetic loci for refractive error and myopia, with identified genes having a wide variety of functions thus indicating multigenic and heterogeneous origin [20,21]. However, the rapid increase in myopia over a single generation is inadequate to significantly change the gene pool and thus suggests a greater effect of gene-environment interactions on myopia [13,22].
- Myopia is commonly detected in the early school years and usually progresses until around 20 years of age [23]. Children with an earlier onset of myopia were found to have a greater rate of progression than children whose onset were later [24]. This effect is magnified in girls, those of Asian descent, and those with a myopic spherical equivalent [24,25]. Some older children and teens may still show myopic progression but, more commonly, this slows down after 12 to 13 years of age [26]. Minimal axial elongation and myopic progression is observed in the third decade of life [27].
Progression of myopia
- Apart from managing the increasing prevalence of myopia, it is also necessary to mitigate the progression to high myopia and its significant risks to ocular health in individuals. Current treatment strategies for myopia progression address the known mechanisms that work by reducing lag of accommodation, reducing defocus of central and peripheral retina, and blocking myopiagenic signaling [28,29].
- 1. Spectacles
- Bifocal spectacle lenses and progressive addition spectacle lenses were widely used to control myopia. The addition of plus lenses was hypothesized to reduce accommodative demand which was thought to stimulate axial elongation [30,31]. Novel spectacle lenses were designed to reduce peripheral hyperopic defocus, another factor hypothesized to increase axial elongation. Several studies have found statistically significant effects with these treatment options [31,32]. However, effects were minimal and were not considered clinically significant [33-36].
- 2. Pharmaceutical agents
- Atropine is a nonselective antimuscarinic and a long-acting mydriatic and cycloplegic agent. Earliest studies for its use in myopia treatment was first reported in the 1970s [37]. Larger randomized controlled trials including ATOM1 and ATOM2 have investigated different concentrations in different degrees of myopia and its effects on refractive error and axial length [38-40]. Although atropine use in the context of myopia is widely investigated and used, the exact mechanism is still unclear [41]. Common practice of atropine use covers a wide range of concentrations from 0.01% to 0.05%, and less commonly, even higher concentrations [42]. There is no current consensus on the optimal concentration and duration to delay myopia progression but higher concentrations were associated with greater adverse effect such as photophobia, loss of accommodation, blurred near vision, and allergic reactions [38,43]. A rebound phenomenon was also found wherein discontinuation of atropine in those with myopia progression of greater than 0.5 D/year required greater concentrations upon resuming treatment [28].
- 3. Behavior
- Several studies suggest that outdoor activity time slows both myopia onset and progression [16,44,45]. In a study comparing time spent outdoors and physical activity as predictors of incident myopia, time spent outdoors had a significantly larger effect [16]. Further investigations suggest that the increased level of vitamin D, dopamine, or ultraviolet light during outdoor activities may be contributory to the mechanism of the observed effect on delaying myopia progression [46-48]. A meta-analysis reported an odds ratio of 0.87 for every additional hour of time spent outdoors each day [49].
- 4. Contact lenses and Ortho-K
- Spectacles and contact lenses are common first line options for myopia correction. They are readily available, well-tolerated, affordable, and provide immediate improvement of vision [13]. Variations in contact lenses which aim to deliver peripheral myopic defocus show evidence in delaying myopia progression [50-52]. This is based on the theory that providing additional positive power in the periphery of these lenses creates a myopic defocus in the peripheral retina, causing reduction in axial growth [14]. The effects of soft multifocal contact lenses have also been studied. In the Bifocal Lenses In Nearsighted Kids (BLINK) study randomized controlled trial, high power add (+2.50D) multifocal lenses compared to medium power add (+1.5D) and single vision lenses reduced the rate of myopia progression over 3 years [53]. Further studies for long-term effectiveness and concerns on myopic rebound are necessary [54]. While these lenses rely on manipulating the optical properties of the eye, Ortho-K uses rigid contact lenses which mechanically change the shape of the cornea to correct myopia and decrease its progression.
Myopia control
- According to unconfirmed stories, the Chinese put small weights on their eyelids during sleep to improve vision [55]. This concept of mechanically altering the shape of the cornea is the cornerstone of the mechanism of Ortho-K. In the 1950s, polymethyl methacrylate (PMMA) contact lenses were introduced. Because of the rigidity of these lenses, unintended changes of corneal curvature and refractive error became evident specially when these lenses were fitted flatter than the corneal curvature [55]. During its inception in the 1960s, Jessen [56] initially described the “orthofocus” technique for reducing myopia methods [56]. Myopes were fitted with PMMA lenses which fit flatter than the corneal curvature and the resulting tear lens corrected the myopia [40]. After removal of these rigid lenses, the flattening effect persisted and allowed improved unaided vision [55]. Early attempts to correct refractive error lacked data on the corneal topography and were generally based on measured refractive error, thus limiting the effect and efficacy of contact lenses [57]. The technique was renamed “orthokeratology” and was accompanied by further clinical studies in the late 1970s. Corneal flattening control was made by changing the base curve and modifying optic zone diameter, peripheral curves of lens [55]. In the 1980s and 1990s, technological breakthroughs gave Ortho-K significant improvements. Rigid gas-permeable (RGP) contact lenses became more widely available. This type of contact lens reduced the risk of corneal hypoxia and edema, addressing a primary concern for contact lenses that required prolonged overnight wear. Increased customization for patients was achieved with computerized corneal topography and computer-driven lathing systems allowing for improved accuracy. Initially, a series of progressively flatter lenses were used until the desired refractive outcome are achieved [58]. Continued developments in modern Ortho-K allowed for increased molding of the corneal surface, allowing for longer intervals between lens changes. A significant development in modern Ortho-K is the use of a reverse geometry design consisting of a central flat area corresponding to the optical zone surrounded by steeper curve. This design became highly favored because it allowed optimized centration and improved tear exchanges [59].
- The U.S. Food and Drug Administration (FDA) approval granted the first approval for an Ortho-K device in 1998 for Contex OK, a rigid RGP for reduction of myopia of up to 3.00D (FDA Summary of Safety and Effectiveness Data: K973697). In 2002, corneal refractive therapy lenses gained FDA approval for myopia of 6.00D with up to 1.75D of astigmatism [60]. In 2019, MiSight (CooperVision, Inc.) gained pre-market FDA approval for myopia correction and decreasing progression in children aged 8 to 12 at the start of treatment (FDA Summary of Safety and Effectiveness Data: PMA P180035). In 2021, the FDA approved to Acuvue Abiliti (Johnson & Johnson Vision Care Inc.) lenses which reports a decrease in myopia of 1.00 D over a 2-year treatment period. Many improvements have been made to the reverse geometry lenses and lens materials are continuously being improved to abate complications [55].
History of Ortho-K
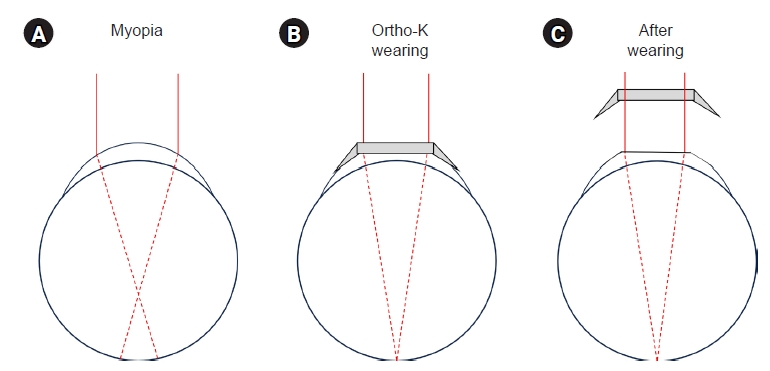
- Ortho-K lenses are rigid contact lenses that work under the premise that overnight wear can alter the corneal surface, making the cornea flatter and thus temporarily reducing myopia in the daytime (Fig. 1) [61]. Although this flattening effect is temporary, many also use Ortho-K lenses to control myopia progression. It is postulated that visual experience affects the growth of the eye and therefore its refractive capacity. Several theories have emerged attributing this effect to factors such as retinal peripheral defocus, corneal higher order aberrations (HOAs), and changes in accommodative response which seem to regulate axial length elongation [62-65].
- 1. Peripheral myopic defocus
- Peripheral retinal defocus occurs when the central focal point is on the retina while the peripheral focal points are not. In peripheral hyperopic defocus, the peripheral focal points are behind the retina while in peripheral myopic defocus they are in front. Animal studies show evidence of peripheral hyperopic defocus stimulating an increase in axial growth [66,67]. It is worth noting that in myopes, the eye is prolate resulting to a greater degree of peripheral hyperopic defocus [68]. To address this, Ortho-K is designed to create peripheral myopic defocus, in turn decreasing or reversing the stimulus for axial elongation.
- MiSight 1 day (omafilcon A; CooperVision, Inc.) is a daily disposable soft contact lens developed for both myopia correction and control of progression. It employs a dual-focus optical design composed of concentric rings with alternating refractive correction zones and peripheral myopic defocus treatment zones. These concentric rings were developed to ensure adequate distance vision as well as peripheral myopic defocus in all gazes. A clinical trial found that use of MiSight slowed axial length growth in treated myopes and, after 6 years of treatment, was found similar to age-matched controls (source 3). Lumb et al. [69] report that these lenses are highly rated in terms of comfort, ease of handling, vision, and satisfaction by children. Although investigations are still underway for this contact lens, the reported outcomes and advantages make it an attractive option for both parents and medical providers [69].
- 2. HOAs and accommodative response
- Apart from peripheral defocus, other HOAs have also been found the affect the regulation of eye growth [70]. HOAs with higher root-mean-square error values lessen accommodative effort and thus decreases the mechanical tension at the equator, leading to slower axial elongation [71]. Some studies reported that more positive spherical aberration and vertical trefoil were associated with less axial growth [71,72]. Ortho-K treatment effectively alters the corneal shape and profile and in turn, increases total HOA that, based on this theory, is desirable in the treatment of myopia progression [73]. Some have attempted to slow axial elongation by using contact lenses that increased spherical aberrations which had modest effects in both children and adults [74]. It is important to note that these lenses induced much smaller spherical aberrations than that of Ortho-K lenses which may not be sufficient to produce the desired effect.
- Similarly, another hypothesized mechanism is the improvement of accommodative response. It has been documented that myopic children have greater accommodative lags than emmetropic children, providing another stimulus for myopia progression. Ortho-K is theorized to improve the accommodative response in myopes [75]. However, studies have inconclusive results [76]. In addition to these effects, the use of Ortho-K has been reported to increase subfoveal choroidal thickness which is usually subnormal in myopic eyes [77]. Although the mechanism remains unclear, it is speculated that the use of Ortho-K induces relaxation of large choroidal vessels, increasing blood supply to support choroidal thickening [60,78].
- 3. Rebound effect
- Although Ortho-K shows a significant slowing effect in myopic progression, the results vary with each report and across individuals. As with other modalities of myopia control, rebound effect after discontinuation is an important concern that should be discussed with the patient. It is unclear whether the effects on myopia control are sustained upon discontinuation. Some have reported the potential for this phenomenon with Ortho-K similar to that seen in atropine use [79-81]. The Discontinuation of Orthokeratology on Eyeball Elongation (DOEE) study reported that discontinuation of Ortho-K use before age 14 years led to an increased rate of axial length elongation. Upon reinstitution of treatment after 6 months, the decrease in myopia progression effect is regained although at a slower rate [79]. This may imply that the use of Ortho-K lenses may need to be continued well past age 14 years to achieve an adequate level of control [63,79]. At present, the optimal duration for an Ortho-K treatment regimen is still unknown. Some clinical trials, such as the Longitudinal Orthokeratology Research in Children (LORIC) [82] and the Retardation of Myopia in Orthokeratology (ROMIO) [52] studies conducted in Hong Kong, were conducted over 2 years and showed promising results in decreasing the rates of axial elongation and myopia progression. Previous studies have also reported greater myopia control in the first 2 years of treatment [52,63]. However, data is limited beyond this period. It is widely accepted that further investigation is necessary to optimize this aspect of treatment.
Mechanism of Ortho-K
- 1. Keratitis
- The primary concern with prolonged overnight contact lens use is corneal health. In particular, this environment reduces the ocular surface defense, changes the epithelial surface integrity, and allows bacterial colonization thus increasing susceptibility to microbial keratitis [83]. Reported rates vary but were found to be similar with daily soft contact lens wear [84]. Poor outcomes are usually based on delayed identification and treatment. Majority of cases show positive microbial cultures, with Acanthamoeba and Pseudomonas aeruginosa being the most common offending agents [85]. Both organisms present with rapidly progressing keratitis, with Acanthamoeba keratitis being particularly severe and sight-threatening, often resulting to corneal scarring [17,81]. Early recognition and prompt treatment is necessary to avert these complications. Associated risk factors for keratitis are similar to those for contact lens use including lack of training on proper hygiene, improper fit, use of tap water, poor compliance, and poor follow-up [86]. Care must be made in educating the patient and their guardians of the importance of compliance to proper lens caring regimen, particularly in the context of Ortho-K which is used overnight. This increased risk of a potentially vision-threatening complication must be discussed with the patient and guardians and must be weighed against the potential benefits.
- 2. Corneal staining, deposits, and lens associated problems
- Corneal staining is most common adverse effect and can present in different patterns with continued Ortho-K use. Some distinctive patterns described are sporadic or diffuse punctate staining, patchy central staining, and whorl-shaped staining [83]. Higher myopia, corneal eccentricity, and smaller corneal horizontal radius can increase the risk of repeated corneal staining episodes [83]. Lens binding is a complication seen with RGPs wherein the contact tear viscosity between the lens and cornea increases during sleep and results in a fluid adhesion force between the two surfaces [87]. Patients may complain that the contact lens feels stuck upon waking up. Forceful removal of the Ortho-K may result in further corneal damage. This may be avoided by using a lubricant before removal. Pigmented ring-shaped corneal deposits resembling Fleischer rings have been reported with Ortho-K use [88,89]. Some suggest that this is caused by stress forces to the epithelium or tear stagnation in the reverse curve area of the lens [88]. It has been reported widely in the Asian population [89] but has also been seen in Caucasian patients [90]. Other lens associated problems are lens tilting and decentration. The treatment zone of Ortho-K lens is important because it compresses the cornea and flatten cornea makes to see well without glasses. Sometimes the factors including increased eyelid tension, corneal astigmatism, movement of lens might cause the lens being out of center [91]. The effort of avoiding this kind of lens associated problems is required before description.
- 3. Other complications
- Other reported but less frequent complications of Ortho-K are bulbar hyperemia, papillary conjunctivitis, corneal edema, palpebral edema, nebular corneal opacity, viral keratoconjunctivitis, band keratopathy, and corneal ulcers. Overall, complications are more common in the first year of use and are less frequent and less severe in children than in adults [92].
Safety
- In Korea, the approximate cost of Ortho-K lenses is USD 1,000. The total cost of treatment increases with each subsequent update or replacement of the lenses after 1 to 2 years. This high cost compared to other treatment modalities like atropine eyedrops may be a financial burden and a barrier to consideration of this treatment.
- With overnight use of Ortho-K, it is imperative that careful and regular follow-up be conducted to ensure corneal health and maintain clean contact lenses. For those prescribing Ortho-K, specialized training, certification, and experience are required to become skillful in optimizing lens fitting and management. For the Ortho-K wearer, aside from knowing the benefits for myopia control, they must also be fully aware of the possible adverse outcomes. Lens care and hygiene are critical for maintaining a healthy cornea and minimizing the potential of complications [83,93].
Considerations with Ortho-K lens prescription
- Although the promising reports regarding Ortho-K use in treatment of myopia, still there are some studies required. Including not only Asian population, but also non-Asians are needed to prove the effect and efficacy of Ortho-K. Further studies are needed about the effective age, period of lens wearing, terms of maximizing stabilization of myopia, potential rebound effect [81]. The education of hand hygiene and warning of safety like corneal infection, opacifications which can cause permanent vision loss. And to evaluate that the effect of Ortho-K is equivalent, noninferior or synergistic effect to low dose atropine on myopia is necessary.
Future of Ortho-K
- Ortho-K is a treatment modality for the correction of myopia and the slowing of its progression. By addressing different mechanisms of myopia progression, Ortho-K has shown promising outcomes. Rapid advances in this technology have improved the efficacy and safety of prolonged use. However, treatment duration for maximum effect still remains unclear. Knowledge of the efficacy, safety profile, and limitations of Ortho-K lenses will be invaluable in guiding treatment decisions for both patients and medical professionals.
Conclusions
-
Conflicts of interest
Changzoo Kim is an editorial board member of the journal but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
-
Funding
None.
-
Author contributions
Conceptualization: SG, CK. Methodology: SG, CK. Investigation: SG, CK. Project administration: CK. Supervision: CK. Writing – original draft: SG, CK. Writing – review & editing: SG, CK.
Article information
- 1. Magnus H. The knowledge of visual disturbances among the Greeks and Romans. Graefes Arch Clin Exp Ophthalmol 1877;23:24–48.
- 2. Hirschberg J. Geschichte der Augenheilkunde. Springer; 1899.
- 3. Kang G, Kim SE. How to write an original article in medicine and medical science. Kosin Med J 2022;37:96–101.ArticlePDF
- 4. Tsai TH, Liu YL, Ma IH, Su CC, Lin CW, Lin LL, et al. Evolution of the prevalence of myopia among taiwanese schoolchildren: a review of survey data from 1983 through 2017. Ophthalmology 2021;128:290–301.ArticlePubMed
- 5. Rim TH, Kim SH, Lim KH, Choi M, Kim HY, Baek SH, et al. Refractive errors in Koreans: the Korea National Health and Nutrition Examination Survey 2008-2012. Korean J Ophthalmol 2016;30:214–24.ArticlePubMedPMCPDF
- 6. Wu LJ, You QS, Duan JL, Luo YX, Liu LJ, Li X, et al. Prevalence and associated factors of myopia in high-school students in Beijing. PLoS One 2015;10:e0120764.ArticlePubMedPMC
- 7. Prabakaran S, Dirani M, Chia A, Gazzard G, Fan Q, Leo SW, et al. Cycloplegic refraction in preschool children: comparisons between the hand-held autorefractor, table-mounted autorefractor and retinoscopy. Ophthalmic Physiol Opt 2009;29:422–6.ArticlePubMed
- 8. Wen G, Tarczy-Hornoch K, McKean-Cowdin R, Cotter SA, Borchert M, Lin J, et al. Prevalence of myopia, hyperopia, and astigmatism in non-Hispanic white and Asian children: multi-ethnic pediatric eye disease study. Ophthalmology 2013;120:2109–16.ArticlePubMed
- 9. Holden BA, Jong M, Davis S, Wilson D, Fricke T, Resnikoff S. Nearly 1 billion myopes at risk of myopia-related sight-threatening conditions by 2050 - time to act now. Clin Exp Optom 2015;98:491–3.ArticlePubMed
- 10. Saw SM, Tong L, Chua WH, Chia KS, Koh D, Tan DT, et al. Incidence and progression of myopia in Singaporean school children. Invest Ophthalmol Vis Sci 2005;46:51–7.ArticlePubMed
- 11. Mutti DO, Mitchell GL, Jones LA, Friedman NE, Frane SL, Lin WK, et al. Axial growth and changes in lenticular and corneal power during emmetropization in infants. Invest Ophthalmol Vis Sci 2005;46:3074–80.ArticlePubMed
- 12. Gordon RA, Donzis PB. Refractive development of the human eye. Arch Ophthalmol 1985;103:785–9.ArticlePubMed
- 13. Baird PN, Saw SM, Lanca C, Guggenheim JA, Smith Iii EL, Zhou X, et al. Myopia. Nat Rev Dis Primers 2020;6:99.ArticlePubMedPDF
- 14. Benavente-Perez A, Nour A, Troilo D. Axial eye growth and refractive error development can be modified by exposing the peripheral retina to relative myopic or hyperopic defocus. Invest Ophthalmol Vis Sci 2014;55:6765–73.ArticlePubMedPMC
- 15. Bez D, Megreli J, Bez M, Avramovich E, Barak A, Levine H. Association between type of educational system and prevalence and severity of myopia among male adolescents in Israel. JAMA Ophthalmol 2019;137:887–93.ArticlePubMed
- 16. Guggenheim JA, Northstone K, McMahon G, Ness AR, Deere K, Mattocks C, et al. Time outdoors and physical activity as predictors of incident myopia in childhood: a prospective cohort study. Invest Ophthalmol Vis Sci 2012;53:2856–65.ArticlePubMedPMC
- 17. Vitale S, Ellwein L, Cotch MF, Ferris FL 3rd, Sperduto R. Prevalence of refractive error in the United States, 1999-2004. Arch Ophthalmol 2008;126:1111–9.ArticlePubMedPMC
- 18. Yusufu M, Wang N. How China is responding to the challenge of myopia. Community Eye Health 2021;34:76.PubMed
- 19. Zhu Z, Chen Y, Tan Z, Xiong R, McGuinness MB, Muller A. Interventions recommended for myopia prevention and control among children and adolescents in China: a systematic review. Br J Ophthalmol 2023;107:160–6.ArticlePubMed
- 20. Baird PN, Schache M, Dirani M. The GEnes in Myopia (GEM) study in understanding the aetiology of refractive errors. Prog Retin Eye Res 2010;29:520–42.ArticlePubMed
- 21. Tedja MS, Haarman AE, Meester-Smoor MA, Kaprio J, Mackey DA, Guggenheim JA, et al. IMI: myopia genetics report. Invest Ophthalmol Vis Sci 2019;60:M89–105.ArticlePubMedPMC
- 22. Chen YP, Hocking PM, Wang L, Povazay B, Prashar A, To CH, et al. Selective breeding for susceptibility to myopia reveals a gene-environment interaction. Invest Ophthalmol Vis Sci 2011;52:4003–11.ArticlePubMed
- 23. Lee SJ, Ahn KS, Yu BC. Determining factors of myopic refractive error in 19 years old men. Kosin Med J 2008;23:66–71.
- 24. Jones-Jordan LA, Sinnott LT, Chu RH, Cotter SA, Kleinstein RN, Manny RE, et al. Myopia progression as a function of sex, age, and ethnicity. Invest Ophthalmol Vis Sci 2021;62:36.Article
- 25. Tricard D, Marillet S, Ingrand P, Bullimore MA, Bourne RRA, Leveziel N. Progression of myopia in children and teenagers: a nationwide longitudinal study. Br J Ophthalmol 2022;106:1104–9.ArticlePubMed
- 26. Jones LA, Mitchell GL, Mutti DO, Hayes JR, Moeschberger ML, Zadnik K. Comparison of ocular component growth curves among refractive error groups in children. Invest Ophthalmol Vis Sci 2005;46:2317–27.ArticlePubMed
- 27. Han X, Guo X, Lee PY, Morgan IG, He M. Six-year changes in refraction and related ocular biometric factors in an adult Chinese population. PLoS One 2017;12:e0183364.ArticlePubMedPMC
- 28. Cooper J, Tkatchenko AV. A review of current concepts of the etiology and treatment of myopia. Eye Contact Lens 2018;44:231–47.ArticlePubMedPMC
- 29. Irving EL, Callender MG, Sivak JG. Inducing myopia, hyperopia, and astigmatism in chicks. Optom Vis Sci 1991;68:364–8.ArticlePubMed
- 30. Mandell RB. Myopia control with bifocal correction. Am J Optom Arch Am Acad Optom 1959;36:652–8.ArticlePubMed
- 31. Fulk GW, Cyert LA, Parker DE. A randomized trial of the effect of single-vision vs. bifocal lenses on myopia progression in children with esophoria. Optom Vis Sci 2000;77:395–401.ArticlePubMed
- 32. Leung JT, Brown B. Progression of myopia in Hong Kong Chinese schoolchildren is slowed by wearing progressive lenses. Optom Vis Sci 1999;76:346–54.ArticlePubMed
- 33. Goss DA. Variables related to the rate of childhood myopia progression. Optom Vis Sci 1990;67:631–6.ArticlePubMed
- 34. Gwiazda J, Thorn F, Held R. Accommodation, accommodative convergence, and response AC/A ratios before and at the onset of myopia in children. Optom Vis Sci 2005;82:273–8.ArticlePubMed
- 35. Sankaridurg P, Donovan L, Varnas S, Ho A, Chen X, Martinez A, et al. Spectacle lenses designed to reduce progression of myopia: 12-month results. Optom Vis Sci 2010;87:631–41.ArticlePubMedPMC
- 36. Edwards MH, Li RW, Lam CS, Lew JK, Yu BS. The Hong Kong progressive lens myopia control study: study design and main findings. Invest Ophthalmol Vis Sci 2002;43:2852–8.PubMed
- 37. Bedrossian RH. The effect of atropine on myopia. Ann Ophthalmol 1971;3:891–7.ArticlePubMed
- 38. Chia A, Lu QS, Tan D. Five-year clinical trial on atropine for the treatment of myopia 2: myopia control with atropine 0.01% eyedrops. Ophthalmology 2016;123:391–9.ArticlePubMed
- 39. Chua WH, Balakrishnan V, Chan YH, Tong L, Ling Y, Quah BL, et al. Atropine for the treatment of childhood myopia. Ophthalmology 2006;113:2285–91.ArticlePubMed
- 40. Chia A, Chua WH, Cheung YB, Wong WL, Lingham A, Fong A, et al. Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology 2012;119:347–54.ArticlePubMed
- 41. Gallego P, Martinez-Garcia C, Perez-Merino P, Ibares-Frias L, Mayo-Iscar A, Merayo-Lloves J. Scleral changes induced by atropine in chicks as an experimental model of myopia. Ophthalmic Physiol Opt 2012;32:478–84.ArticlePubMed
- 42. Wildsoet CF, Chia A, Cho P, Guggenheim JA, Polling JR, Read S, et al. IMI - Interventions myopia institute: interventions for controlling myopia onset and progression report. Invest Ophthalmol Vis Sci 2019;60:M106–31.ArticlePubMed
- 43. Gong Q, Janowski M, Luo M, Wei H, Chen B, Yang G, et al. Efficacy and adverse effects of atropine in childhood myopia: a meta-analysis. JAMA Ophthalmol 2017;135:624–30.ArticlePubMedPMC
- 44. Rose KA, Morgan IG, Ip J, Kifley A, Huynh S, Smith W, et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology 2008;115:1279–85.ArticlePubMed
- 45. He M, Xiang F, Zeng Y, Mai J, Chen Q, Zhang J, et al. Effect of time spent outdoors at school on the development of myopia among children in China: a randomized clinical trial. JAMA 2015;314:1142–8.ArticlePubMed
- 46. Mutti DO, Marks AR. Blood levels of vitamin D in teens and young adults with myopia. Optom Vis Sci 2011;88:377–82.ArticlePubMedPMC
- 47. Zhou X, Pardue MT, Iuvone PM, Qu J. Dopamine signaling and myopia development: what are the key challenges. Prog Retin Eye Res 2017;61:60–71.ArticlePubMedPMC
- 48. Rose KA, French AN, Morgan IG. Environmental factors and myopia: paradoxes and prospects for prevention. Asia Pac J Ophthalmol (Phila) 2016;5:403–10.PubMed
- 49. Sherwin JC, Reacher MH, Keogh RH, Khawaja AP, Mackey DA, Foster PJ. The association between time spent outdoors and myopia in children and adolescents: a systematic review and meta-analysis. Ophthalmology 2012;119:2141–51.ArticlePubMed
- 50. Cheng D, Woo GC, Drobe B, Schmid KL. Effect of bifocal and prismatic bifocal spectacles on myopia progression in children: three-year results of a randomized clinical trial. JAMA Ophthalmol 2014;132:258–64.ArticlePubMed
- 51. Gwiazda J, Hyman L, Hussein M, Everett D, Norton TT, Kurtz D, et al. A randomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in children. Invest Ophthalmol Vis Sci 2003;44:1492–500.ArticlePubMed
- 52. Cho P, Cheung SW. Retardation of Myopia in Orthokeratology (ROMIO) study: a 2-year randomized clinical trial. Invest Ophthalmol Vis Sci 2012;53:7077–85.ArticlePubMed
- 53. Walline JJ, Walker MK, Mutti DO, Jones-Jordan LA, Sinnott LT, Giannoni AG, et al. Effect of high add power, medium add power, or single-vision contact lenses on myopia progression in children: the BLINK Randomized Clinical Trial. JAMA 2020;324:571–80.ArticlePubMedPMC
- 54. Berntsen DA, Sinnott LT, Mutti DO, Zadnik K. A randomized trial using progressive addition lenses to evaluate theories of myopia progression in children with a high lag of accommodation. Invest Ophthalmol Vis Sci 2012;53:640–9.ArticlePubMedPMC
- 55. Swarbrick HA. Orthokeratology review and update. Clin Exp Optom 2006;89:124–43.ArticlePubMed
- 56. Jessen GN. Contact lenses as a therapeutic device. Am J Optom Arch Am Acad Optom 1964;41:429–35.ArticlePubMed
- 57. Lui WO, Edwards MH, Cho P. Contact lenses in myopia reduction: from orthofocus to accelerated orthokeratology. Cont Lens Anterior Eye 2000;23:68–76.ArticlePubMed
- 58. Nti AN, Berntsen DA. Optical changes and visual performance with orthokeratology. Clin Exp Optom 2020;103:44–54.ArticlePubMedPDF
- 59. Charm J. Orthokeratology: clinical utility and patient perspectives. Clin Optom (Auckl) 2017;9:33–40.ArticlePubMedPMC
- 60. Lipson MJ, Brooks MM, Koffler BH. The role of orthokeratology in myopia control: a review. Eye Contact Lens 2018;44:224–30.ArticlePubMed
- 61. Swarbrick HA, Alharbi A, Watt K, Lum E, Kang P. Myopia control during orthokeratology lens wear in children using a novel study design. Ophthalmology 2015;122:620–30.ArticlePubMed
- 62. Cho P, Tan Q. Myopia and orthokeratology for myopia control. Clin Exp Optom 2019;102:364–77.ArticlePubMedPDF
- 63. Vincent SJ, Cho P, Chan KY, Fadel D, Ghorbani-Mojarrad N, Gonzalez-Meijome JM, et al. CLEAR: orthokeratology. Cont Lens Anterior Eye 2021;44:240–69.ArticlePubMed
- 64. Wu J, Fang W, Xu H, Liu X, Zhao D, Rong Q. The biomechanical response of the cornea in orthokeratology. Front Bioeng Biotechnol 2021;9:743745.ArticlePubMedPMC
- 65. Kim SJ, Lee JE. Influence of orthokeratology lens on axial length elongation and myopic progression in childhood myopia. Kosin Med J 2017;32:204–11.ArticlePDF
- 66. Smith EL 3rd, Hung LF, Huang J. Relative peripheral hyperopic defocus alters central refractive development in infant monkeys. Vision Res 2009;49:2386–92.ArticlePubMedPMC
- 67. Irving EL, Callender MG, Sivak JG. Inducing ametropias in hatchling chicks by defocus: aperture effects and cylindrical lenses. Vision Res 1995;35:1165–74.ArticlePubMed
- 68. Mutti DO, Sholtz RI, Friedman NE, Zadnik K. Peripheral refraction and ocular shape in children. Invest Ophthalmol Vis Sci 2000;41:1022–30.PubMed
- 69. Lumb E, Sulley A, Logan NS, Jones D, Chamberlain P. Six years of wearer experience in children participating in a myopia control study of MiSight® 1 day. Cont Lens Anterior Eye 2023;46:101849.ArticlePubMed
- 70. Karimian F, Feizi S, Doozande A. Higher-order aberrations in myopic eyes. J Ophthalmic Vis Res 2010;5:3–9.PubMedPMC
- 71. Hiraoka T, Kotsuka J, Kakita T, Okamoto F, Oshika T. Relationship between higher-order wavefront aberrations and natural progression of myopia in schoolchildren. Sci Rep 2017;7:7876.ArticlePubMedPMCPDF
- 72. Lau JK, Vincent SJ, Collins MJ, Cheung SW, Cho P. Ocular higher-order aberrations and axial eye growth in young Hong Kong children. Sci Rep 2018;8:6726.ArticlePubMedPMCPDF
- 73. Gifford P, Li M, Lu H, Miu J, Panjaya M, Swarbrick HA. Corneal versus ocular aberrations after overnight orthokeratology. Optom Vis Sci 2013;90:439–47.ArticlePubMed
- 74. Allen PM, Radhakrishnan H, Rae S, Calver RI, Theagarayan BP, Nelson P, et al. Aberration control and vision training as an effective means of improving accommodation in individuals with myopia. Invest Ophthalmol Vis Sci 2009;50:5120–9.ArticlePubMed
- 75. Summers JA. The choroid as a sclera growth regulator. Exp Eye Res 2013;114:120–7.ArticlePubMedPMC
- 76. Felipe-Marquez G, Nombela-Palomo M, Cacho I, Nieto-Bona A. Accommodative changes produced in response to overnight orthokeratology. Graefes Arch Clin Exp Ophthalmol 2015;253:619–26.ArticlePubMedPDF
- 77. Chen Z, Xue F, Zhou J, Qu X, Zhou X. Effects of orthokeratology on choroidal thickness and axial length. Optom Vis Sci 2016;93:1064–71.ArticlePubMed
- 78. Li Z, Cui D, Hu Y, Ao S, Zeng J, Yang X. Choroidal thickness and axial length changes in myopic children treated with orthokeratology. Cont Lens Anterior Eye 2017;40:417–23.ArticlePubMed
- 79. Cho P, Cheung SW. Discontinuation of orthokeratology on eyeball elongation (DOEE). Cont Lens Anterior Eye 2017;40:82–7.ArticlePubMed
- 80. Wang M, Cui C, Sui Y, Yu SA, Ma JX, Fu AC. Effect of 0.02% and 0.01% atropine on astigmatism: a two-year clinical trial. BMC Ophthalmol 2022;22:161.ArticlePubMedPMCPDF
- 81. VanderVeen DK, Kraker RT, Pineles SL, Hutchinson AK, Wilson LB, Galvin JA, et al. Use of orthokeratology for the prevention of myopic progression in children: a report by the American Academy of Ophthalmology. Ophthalmology 2019;126:623–36.ArticlePubMed
- 82. Cho P, Cheung SW, Edwards M. The longitudinal orthokeratology research in children (LORIC) in Hong Kong: a pilot study on refractive changes and myopic control. Curr Eye Res 2005;30:71–80.ArticlePubMed
- 83. Liu YM, Xie P. The safety of orthokeratology: a systematic review. Eye Contact Lens 2016;42:35–42.ArticlePubMed
- 84. Santodomingo-Rubido J. Foreword: orthokeratology for myopia control in everyday practice. Cont Lens Anterior Eye 2023;46:101798.ArticlePubMed
- 85. Kam KW, Yung W, Li GK, Chen LJ, Young AL. Infectious keratitis and orthokeratology lens use: a systematic review. Infection 2017;45:727–35.ArticlePubMedPDF
- 86. Watt KG, Swarbrick HA. Trends in microbial keratitis associated with orthokeratology. Eye Contact Lens 2007;33(6 Pt 2):373–82.ArticlePubMed
- 87. Chan B, Cho P, Cheung SW. Orthokeratology practice in children in a university clinic in Hong Kong. Clin Exp Optom 2008;91:453–60.ArticlePubMed
- 88. Cho P, Chui WS, Mountford J, Cheung SW. Corneal iron ring associated with orthokeratology lens wear. Optom Vis Sci 2002;79:565–8.ArticlePubMed
- 89. Cho P, Chui WS, Cheung SW. Reversibility of corneal pigmented arc associated with orthokeratology. Optom Vis Sci 2003;80:791–5.ArticlePubMed
- 90. Gonzalez-Meijome JM, Gonzalez-Perez J, Garcia-Porta N, Diaz-Rey A, Parafita-Mato MA. Pigmented corneal ring associated with orthokeratology in Caucasians: case reports. Clin Exp Optom 2012;95:548–52.ArticlePubMed
- 91. Sun L, Li ZX, Chen Y, He ZQ, Song HX. The effect of orthokeratology treatment zone decentration on myopia progression. BMC Ophthalmol 2022;22:76.ArticlePubMedPMCPDF
- 92. Gispets J, Yebana P, Lupon N, Cardona G, Perez-Corral J, Paune J, et al. Efficacy, predictability and safety of long-term orthokeratology: an 18-year follow-up study. Cont Lens Anterior Eye 2022;45:101530.ArticlePubMed
- 93. Lo J, Kuo MT, Chien CC, Tseng SL, Lai YH, Fang PC. Microbial bioburden of orthokeratology contact lens care system. Eye Contact Lens 2016;42:61–7.ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite
