KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Epub ahead of print > Article
-
Case report
Cardiovascular collapse during transcatheter aortic valve replacement in monitored anesthesia care using an end-tidal carbon dioxide monitor: a case report -
Wonjin Lee
 , Jaewoo Suh
, Jaewoo Suh -
>
Epub ahead of print
DOI: https://doi.org/10.7180/kmj.23.134
Published online: January 2, 2024
Department of Anesthesiology and Pain Medicine, Inje University Busan Paik Hospital, Inje University of College of Medicine, Busan, Korea
- Corresponding Author: Wonjin Lee, MD Department of Anesthesiology and Pain Medicine, Inje University Busan Paik Hospital, Inje University of College of Medicine, 75 Bokji-ro, Busanjin-gu, Busan 47392, Korea Tel: +82-51-890-6520 Fax: +82-51-898-4216 E-mail: 2wonjin@naver.com
Copyright © 2024 Kosin University College of Medicine.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 232 Views
- 3 Download
Abstract
- Capnography is commonly used to monitor respiration during general anesthesia. However, it has limited utility in patients with respiratory distress during sedation. This case report examines capnography use in a transcatheter aortic valve replacement procedure performed on an elderly woman with severe aortic stenosis. A 73-year-old woman with a history of non-ST-elevation myocardial infarction and congenital heart failure presented with severe dyspnea caused by severe aortic stenosis. Transcatheter aortic valve replacement was preferred over surgery due to her comorbidities. Monitored anesthesia care was administered with a capnogram. During the procedure, the patient was sedated with remimazolam, maintaining a bispectral index range of 60–80 and a score of 2 on the Modified Observer’s Assessment of Alertness/Sedation scale. Although irregular breathing patterns and a gradual decrease in oxygen saturation were observed following remimazolam infusion, the patient’s respiration eventually stabilized. However, the patient experienced cardiovascular collapse 45 minutes after sedation began. The arterial carbon dioxide pressure measured by arterial blood gas analysis performed just before resuscitation was 68.4 mmHg. After one cycle of resuscitation, the patient recovered. The procedure was successfully performed under general anesthesia, which was replaced with monitored anesthesia care during resuscitation. Although most monitoring devices have similar utility for both general anesthesia and sedation, capnography has limitations for evaluating respiration during sedation, especially for patients with respiratory distress. Therefore, anesthesiologists or medical staff who provide sedation should not neglect periodical arterial carbon dioxide pressure observations via other methods, such as arterial blood gas analysis.
- Capnography is a device used to evaluate a patient’s respiration. Its use has increased as the demand for anesthesia outside operating units has greatly expanded. This monitoring technique can help anesthesiologists evaluate the presence and quality of respiration. However, applying an end-tidal carbon dioxide (EtCO2) monitor for particular patients might be less valuable. In this case report, we discuss a woman who received a transcatheter aortic valve replacement in an interventional radiology suite.
Introduction
- Ethical statement: This study was exempted from review by the Institutional Review Board (IRB) of Busan Paik Hospital, Inje University of College of Medicine (IRB No: 2023-03-012-001). Informed consent was waived.
- A 73-year-old woman (144 cm, 40 kg) previously diagnosed with non-ST-elevation myocardial infarction and congenital heart failure 20 years prior was admitted to the emergency department due to dyspnea. Physical examination revealed severe dyspnea, classified as New York Heart Association class 4. Transesophageal echocardiography confirmed severe aortic stenosis and moderate aortic regurgitation. Additionally, the patient had mild to moderate mitral and tricuspid regurgitation and moderate pulmonary hypertension. Pulmonary function tests indicated restrictive lung disease, which caused pulmonary edema and bilateral pleural effusion observed as extensive peribronchovascular consolidation with ground glass opacity and interlobular thickening in an unenhanced chest computed tomography scan. Considering her age, physical examination results, and imaging findings, the short-term risk for open cardiac surgery was 10%, which was too high for a surgical aortic valve replacement. A collaborative heart valve team consisting of cardiologists and thoracic surgeons decided to perform transcatheter aortic intervention.
- The anesthesiologists and cardiologists determined that monitored anesthesia care would be the optimal choice based on its association with reduced 30-day mortality, shorter hospital stays, and impracticality of extubation [1]. We applied an automatic blood pressure cuff, electrocardiogram, and pulse oximetry for basic monitoring. We attached a bispectral index signal (BIS) monitor to assess sedation level and non-rebreather oxygen mask with a reservoir bag (#0562 Adult CO2/O2 Sampling Mask, Westme), which allowed side-stream capnograph monitoring with a ventilator (Primus, Drägerwerk AG & Co. KGaA). To prevent air leakage from the gap between the mask and face, we adjusted the nose clip and used silicon tape (Innomed silicone tape, Chinoomed) around the mask. Moreover, the patient’s neck was extended with a pillow to maintain airway patency. After the reservoir back was full of 100% oxygen, the oxygen flow was adjusted to 6 L/min. Despite gradual decrease in saturation at the beginning of sedation, oxygen saturation was maintained at 100% during the procedure.
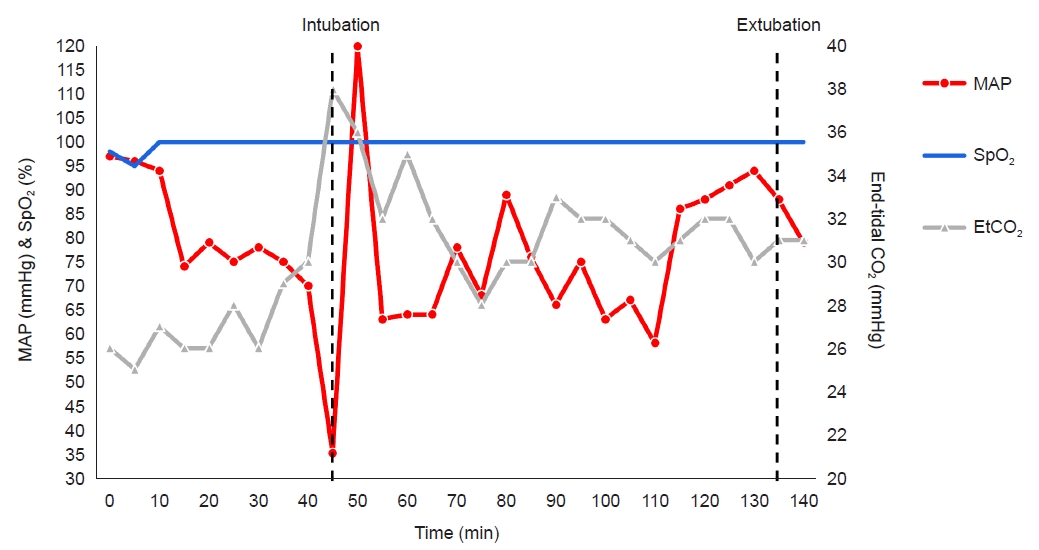
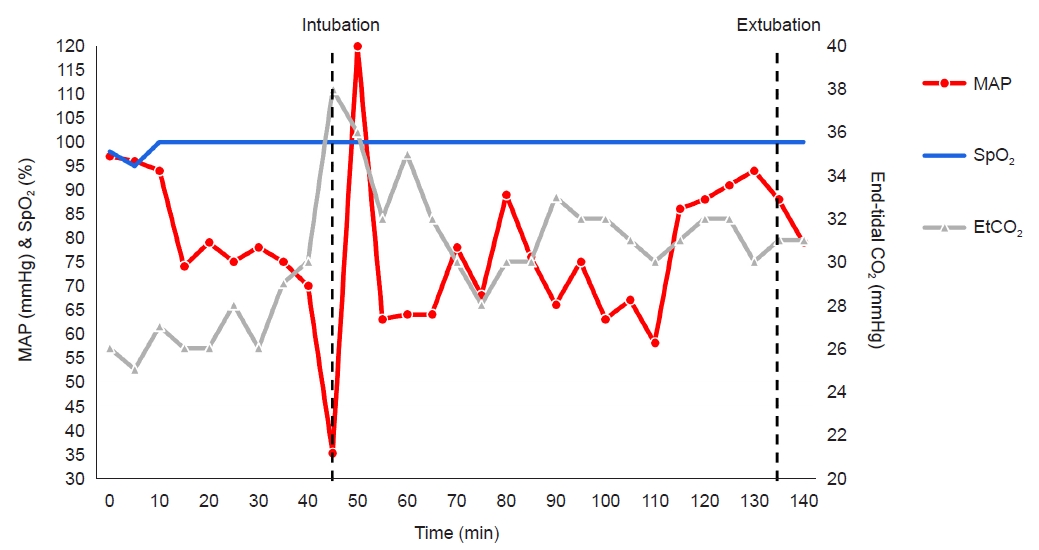
- Remimazolam was administered for sedation, with a loading dose of 6 mg/kg/hr over 3 minutes, followed by a maintenance dose of 0.3 mg/kg/hr after the Modified Observer’s Assessment of Alertness/Sedation scale (MOAA/S) reached 2 [2,3]. The BIS range was 60–80. We used remifentanil by the target site infusion method with the Minto model for pain reduction during the procedure, initially targeted at 0.8 ng/cc of an effect-site concentration and maintained at 1.0 ng/cc of effect-site concentration at which self-respiration was well maintained. To manage a sudden drop in blood pressure during rapid ventricular pacing, arterial line, and central venous catheter were inserted. The mean arterial blood pressure (MAP) was maintained above 75 mmHg, and respiration rate measured by capnogram remained regular at 10 breaths/min, with EtCO2 levels at 25–30 mmHg.
- We sampled the arterial blood to determine why the arterial blood pressure gradually decreased 45 minutes after sedation began. The pH of the arterial blood was 7.17, and the arterial carbon dioxide pressure (PaCO2) and actual bicarbonate were 68.4 mmHg and 22.4 mmol/L, respectively. While we tried to wake the patient to encourage deep breathing, the MAP dropped below 40 mmHg, and the patient was pulseless, triggering resuscitation (Fig. 1). During resuscitation, the patient was intubated following 50 mg of rocuronium injection and general anesthesia was maintained by sevoflurane. Hyperventilation was applied to reduce PaCO2. Following the conversion from monitored anesthesia care to general anesthesia, the EtCO2 level was 38 mmHg. The patient recovered from cardiopulmonary collapse after one cycle of resuscitation. Arterial blood gas analysis (ABGA) improved (pH 7.31; PaCO2 44.9 mmHg; actual bicarbonate 22.4 mmol/L) without a sodium bicarbonate injection. The procedure finished successfully, and we extubated the patient after confirmation that ABGA was normal (pH 7.46; PaCO2 32.9 mmHg; actual bicarbonate 23.6 mmol/L) (Table. 1).
Case report
- EtCO2 monitoring is an essential component of general anesthesia and is recommended for evaluating respiration during sedation [4]. It enables anesthesiologists to detect the absence of respiration more quickly than pulse oximetry and provides information on the PaCO2 level. However, these advantages are most effective for mechanically ventilated patients, limiting the utility of EtCO2 monitoring to that specific population [5].
- Mehta et al. [6] investigated the sensitivity of EtCO2, an indirect measure of respiration, in relation to minute volume, which serves as a direct measurement of ventilation, three groups were compared: patients under general anesthesia, individuals undergoing procedural sedation, and awake volunteers. The procedural sedation group exhibited lower sensitivity than other groups, indicating that minute volume changed less in relation to EtCO2 levels in that group [7].
- Sedation may result in a dampened respiratory drive. The low sensitivity may be attributed to the blunting of the respiratory drive, which typically responds to elevated CO2 levels and is regulated by central and peripheral chemoreceptor activation. Additionally, sensitivity demonstrates a bimodal distribution, with higher sensitivity observed when the depth of sedation approaches that of general anesthesia or while awake [6]. It has been observed that BIS does not reliably indicate the depth of sedation when using remimazolam [8]. Although no intraoperative awareness was reported with a BIS score of 60 or higher during remimazolam administration for general anesthesia, it does not assure definite depth of the sedation [9]. Therefore, it is recommended to evaluate the depth of sedation using additional assessment tools like the MOAA/S scale to ensure more accurate results [2].
- Herein, the patient received sedation with remimazolam, maintaining a BIS range of 60–80 and MOAA/S 2 [2,8]. Despite remimazolam having comparable efficacy and safety to propofol [2], irregular breathing patterns were observed following its initiation. Although the regularity of respiration stabilized soon after, the depth of sedation may have been intermediate, resulting in a lower sensitivity of EtCO2 monitoring. Considering these factors, general anesthesia would be preferable to maximize the sensitivity of EtCO2 monitoring.
- EtCO2 monitoring is further constrained by challenges associated with predicting PaCO2 based on EtCO2 measurements. Limited studies have demonstrated the usefulness of EtCO2 monitoring as a predictor of PaCO2. However, these studies only analyzed patients with acute asthma attacks, not those with respiratory distress like chronic obstructive pulmonary disease, pneumonia, and congestive heart failure. Also, they used less effective methods to measure the concordance between two factors [10,11]. When using the Bland and Altman plot analysis, the golden standard, EtCO2 monitoring, showed limited effectiveness in predicting PaCO2 in patients with respiratory distress [5].
- The observed limitations in predicting PaCO2 using EtCO2 in patients with respiratory distress can be attributed to several factors. First, patients in respiratory distress often exhibit increased physiologic and pathologic dead space compared to healthy individuals. This results in a ventilation-perfusion mismatch, which impairs gas exchange between the alveoli and capillary arteries. Furthermore, shallow and rapid breathing patterns associated with respiratory distress may not allow adequate exhalation, leading to decrease in functional residual capacity. Consequently, the gradient between EtCO2 and PaCO2 was elevated. Although it was difficult to state that the patient who had several cardiopulmonary diseases, had shallow breath because of limited data about minute volume, these underlying conditions might contribute to weakened breathing and a significant degree in ventilation-perfusion mismatch, further complicating the prediction of PaCO2 using EtCO2 measurements.
- According to the clinical practice guidelines for diagnostic and procedural sedation [12], EtCO2 monitoring is recommended for preventing hypoxia during sedation. In this context, the application of EtCO2 monitoring for our patient was effective in ensuring adequate oxygenation. However, the patient experienced cardiovascular collapse and demonstrated hypercapnia. The EtCO2 and PaCO2 gradient exceeded 30 mmHg, surpassing the acceptable limit [5]. This emphasizes the importance of not mistaking adequate oxygenation for effective CO2 elimination. While the cardiovascular collapse in our case was likely due to inadequate exhalation of CO2, it is possible that the excessive infusion of remimazolam from the beginning of the sedation might have been the underlying cause of the collapse. However, though remimazolam could induce not only respiratory regression but mild depression of mean blood pressure, the amount of remimazolam, infused up to cardiovascular collapse, was not even enough for the depression which was shown in the study [3].
- The CO2 retention in this case may have originated by anesthesiologists relying on EtCO2, thought to reflect respiration during sedation. Other monitoring devices have similar utility in both general anesthesia and sedation. However, during sedation, EtCO2 monitors are limited in evaluating the adequacy of a patient’s respiration under respiratory distress. Therefore, medical staff providing sedation should not neglect periodical PaCO2 evaluation by other means, such as ABGA.
Discussion
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Acknowledgments
The authors thank Seung Bae Cho, MD (Inje University Busan Paik Hospital, Inje University of College of Medicine, Busan, Korea) for intensive editing.
-
Funding
None.
-
Author contributions
Conceptualization: JS, WL. Data curation: JS. Supervision: WL. Validation: WL. Writing-original draft: JS. Writing-review & editing: JS.
Article information
- 1. Butala NM, Chung M, Secemsky EA, Manandhar P, Marquis-Gravel G, Kosinski AS, et al. Conscious sedation versus general anesthesia for transcatheter aortic valve replacement: variation in practice and outcomes. JACC Cardiovasc Interv 2020;13:1277–87.ArticlePubMedPMC
- 2. Kim KM. Remimazolam: pharmacological characteristics and clinical applications in anesthesiology. Anesth Pain Med (Seoul) 2022;17:1–11.ArticlePubMedPMCPDF
- 3. Morimoto Y. Efficacy and safety profile of remimazolam for sedation in adults undergoing short surgical procedures. Ther Clin Risk Manag 2022;18:95–100.ArticlePubMedPMCPDF
- 4. American Society of Anesthesiologists (ASA). Standards for basic anesthetic monitoring [Internet]. ASA; c2020 [cited 2023 May 25]. https://www.asahq.org/standards-and-guidelines/standards-for-basic-anesthetic-monitoring
- 5. Jabre P, Jacob L, Auger H, Jaulin C, Monribot M, Aurore A, et al. Capnography monitoring in nonintubated patients with respiratory distress. Am J Emerg Med 2009;27:1056–9.ArticlePubMed
- 6. Mehta JH, Williams GW 2nd, Harvey BC, Grewal NK, George EE. The relationship between minute ventilation and end tidal CO2 in intubated and spontaneously breathing patients undergoing procedural sedation. PLoS One 2017;12:e0180187.ArticlePubMedPMC
- 7. Ortega R, Connor C, Kim S, Djang R, Patel K. Monitoring ventilation with capnography. N Engl J Med 2012;367:e27.ArticlePubMed
- 8. Chae D, Kim HC, Song Y, Choi YS, Han DW. Pharmacodynamic analysis of intravenous bolus remimazolam for loss of consciousness in patients undergoing general anaesthesia: a randomised, prospective, double-blind study. Br J Anaesth 2022;129:49–57.ArticlePubMed
- 9. Choi BM, Lee JS, Kim KM, Bang JY, Lee EK, Noh GJ. Frequency and characteristics of patients with bispectral index values of 60 or higher during the induction and maintenance of general anesthesia with remimazolam. Sci Rep 2023;13:9992.ArticlePubMedPMCPDF
- 10. Corbo J, Bijur P, Lahn M, Gallagher EJ. Concordance between capnography and arterial blood gas measurements of carbon dioxide in acute asthma. Ann Emerg Med 2005;46:323–7.ArticlePubMed
- 11. Yosefy C, Hay E, Nasri Y, Magen E, Reisin L. End tidal carbon dioxide as a predictor of the arterial PCO2 in the emergency department setting. Emerg Med J 2004;21:557–9.ArticlePubMedPMC
- 12. The Korean Society of Anesthesiologists. Does the measurement of end-tidal carbon dioxide, added to standardized monitoring device for the adult patient during sedation, decrease hypoxia? In: The Korean Society of Anesthesiologists. Clinical Practice Guidelines for Diagnostic and Procedural Sedation. 1st ed. Yeomungak Press; 2022. p. 167-82.
 PubReader
PubReader ePub Link
ePub Link Cite
Cite