KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Volume 39(1); 2024 > Article
-
Original article
Effects of cholecalciferol and omega-3 fatty acids on hepcidin levels in 5/6 nephrectomy rats -
Yu In Jeong1
 , Hyo Jin Jung1, Mi Hwa Lee2, Young Ki Son1, Seong Eun Kim1, Won Suk An1,3,*, Su Mi Lee1,*
, Hyo Jin Jung1, Mi Hwa Lee2, Young Ki Son1, Seong Eun Kim1, Won Suk An1,3,*, Su Mi Lee1,* -
Kosin Medical Journal 2024;39(1):35-43.
DOI: https://doi.org/10.7180/kmj.23.137
Published online: September 25, 2023
1Department of Internal Medicine, Dong-A University College of Medicine, Busan, Korea
2Department of Anatomy and Cell Biology, Dong-A University, Busan, Korea
3Medical Science Research Center, Dong-A University, Busan, Korea
- Corresponding Author: Su Mi Lee, MD, PhD Department of Internal Medicine, Dong-A University College of Medicine, 26 Daesingongwon-ro, Seo-gu, Busan 49201, Korea Tel: +82-51-240-2837 Fax: +82-51-242-5974 E-mail: sumilee@dau.ac.kr
- Corresponding Author: Won Suk An, MD, PhD Department of Internal Medicine, Dong-A University College of Medicine, 26 Daesingongwon-ro, Seo-gu, Busan 49201, Korea Tel: +82-51-240-2811 Fax: +82-51-242-5852 E-mail: anws@dau.ac.kr
- *These authors contributed equally to this work as corresponding authors.
© 2024 Kosin University College of Medicine.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,120 Views
- 15 Download
Abstract
-
Background
- Anemia is a common complication of chronic kidney disease (CKD). In patients with CKD-related anemia, an inverse relationship between vitamin D and hepcidin levels has been observed. Hepcidin is a key regulator of iron homeostasis, mediated via binding to ferroportin. The aim of this study was to investigate the effects of cholecalciferol and omega-3 fatty acids (FA) on hepcidin levels using 5/6 nephrectomized (Nx) rats.
-
Methods
- Male Sprague-Dawley rats were divided into five groups: sham control, 5/6 Nx, 5/6 Nx treated with cholecalciferol, 5/6 Nx treated with omega-3 FA, and 5/6 Nx treated with both cholecalciferol and omega-3 FA. We measured the hepcidin and ferroportin levels in the kidney and liver by enzyme-linked immunosorbent assays and Western blots. We evaluated hepcidin expression in the kidney by immunohistochemical staining.
-
Results
- Among the five groups, 5/6 Nx rats exhibited the worst kidney function. Compared with the sham controls, 5/6 Nx rats showed significantly increased serum hepcidin levels and decreased vitamin D levels. Supplementation with either omega-3 FA or cholecalciferol decreased hepcidin and increased vitamin D levels, with a concurrent improvement of anemia. Furthermore, 5/6 Nx rats treated with omega-3 FA/cholecalciferol showed decreased ferroportin and ferritin levels, while iron and total iron-binding capacity levels increased.
-
Conclusions
- Treatment with a combination of cholecalciferol and omega-3 FA may improve anemia in a CKD rat model by decreasing hepcidin levels.
- Anemia is a common complication of chronic kidney disease (CKD). According to the Kidney Disease: Improving Global Outcomes guidelines, anemia is defined as a hemoglobin level less than 13.0 g/dL in men and 12.0 g/dL in women. In patients with CKD, the frequency of anemia is twice as high as in the general population [1,2]. This anemic condition is associated with a decreased quality of life, exacerbated kidney function, increased risk of mortality, and cardiovascular complications [3-6]. The incidence of anemia in CKD is 8.4% in stage 1, 12% in stage 2, 17% in stage 3, and more than 50% in stages 4 and 5 [1].
- The occurrence of anemia in patients with CKD may be caused by a reduction in erythropoietin production due to decreased kidney function, iron deficiency, inflammation, and the accumulation of uremic toxins [7]. Vitamin D deficiency is one of the lesser-known causes of anemia in CKD and is inversely correlated with the prevalence of anemia [8-10].
- Hepcidin, a small peptide produced by the liver, is a key regulator of iron homeostasis via binding to ferroportin on the membrane of enterocytes, macrophages, and erythroid cells [11]. When hepcidin binds to ferroportin, it inhibits both the intestinal iron absorption and the iron release from macrophages and hepatocytes. In patients with CKD, hepcidin levels increase with a decline in renal function [12] with an inverse relationship between vitamin D and hepcidin levels [13]. The supplementation of omega-3 fatty acids (FA) increases hemoglobin levels in patients undergoing peritoneal dialysis [14]. In obese children, both the iron and hepcidin levels were improved after omega-3 FA supplementation [15].
- The aim of this study was to investigate the effect of cholecalciferol and omega-3 FA supplementation on iron homeostasis mediated via regulation of the hepcidin levels using 5/6 nephrectomized (Nx) rats. We also evaluated hepcidin expression in the kidney.
Introduction
- Ethical statements: All procedures involving animals were performed in accordance with the approval of the Dong-A University Institutional Animal Care Committee (IACUC-14-4).
- 1. Experimental design
- In this study, we report additional data obtained from the same nephrectomy rats used in a previously published study [16]. The rats were randomized to five groups (n=6 for each group) and treated for 45 days: sham control rats maintained on saline (1 mL/kg/day by gastric lavage), 5/6 Nx rats treated with saline (1 mL/kg/day by gastric lavage); 5/6 Nx rats treated with vitamin D by gastric lavage (cholecalciferol 3,000 IU/kg/wk; Solgar); 5/6 Nx rats treated with omega-3 FA by gastric lavage (Omacor 300 mg/kg/day; Pronova Biocare); 5/6 Nx rats treated with cholecalciferol/omega-3 FA. The dose and usage of omega-3 FAs containing 460 mg of eicosapentaenoic acid and 380 mg of docosahexaenoic acid per gram of Omacor were determined in a previous study [17].
- 2. Biochemical evaluation
- Hemoglobin levels were assessed in the K3EDTA-treated whole blood using a HemoCue Hemoglobin 201 analyzer. Serum hepcidin and erythropoietin levels were measured using enzyme-linked immunosorbent assay (ELISA) kits (DRG instruments GmbH and CusaBio Biotech Co.). Serum iron and unsaturated iron-binding capacity levels were measured using a colorimetric method (JalCA). The total serum iron and unsaturated iron-binding capacity levels were defined as the total iron-binding capacity (TIBC). Serum ferritin and ferroportin levels were measured with rat-specific ELISA kits (Abcam and Cloud-Clone Corp.). Serum interleukin-6 (IL-6) levels were measured with a rat-specific Quantikine ELISA kit from R&D Systems. Serum 25-hydroxyvitamin D [25(OH)D] and 1,25-dihydroxyvitamin D [1,25(OH)2D] levels were measured using a radioimmunoassay kit (DiaSorin Inc.).
- 3. Immunohistochemical analyses
- Histologic evaluation and immunohistochemistry were performed as previously described [16]. Briefly, the kidney was fixed in 10% buffered formalin, followed by embedding in paraffin wax after sacrificing the rats. The kidney was cut into 4 μm serial sections, which were transferred into a sodium citrate buffer (10 mM Sodium Citrate, 0.05% Tween20, pH 6.0). The slides were then microwaved on medium power for 20 minutes for antigen retrieval. To block endogenous peroxidase activity, the tissue sections were incubated with 0.3% H2O2 in phosphate-buffered saline for 30 minutes. The slides were then blocked with 5% normal goat serum for 1 hour at room temperature, and incubated first with the anti-hepcidin antibody at 4 ℃ overnight and then with a secondary antibody for 1 hour at 37 ℃. Finally, slides were stained with 3,3-diaminobenzidine, its H2O2 substrate, and hematoxylin. All sections were analyzed using a 3DHISTECH Panoramic MIDI (3DHISTECH Ltd) microscope, at x200 magnification.
- 4. Western blot analysis
- Western blot analysis was conducted as previously described with slight modifications [16]. Briefly, kidney and liver tissues were lysed using PRO-PREP protein extraction solution (Intron biotechnology), and centrifuged at 14,000 rpm for 20 minutes at 4 °C. The protein concentrations of the lysates were determined using Bradford protein assay reagent (Bio-Rad), according to the manufacturer’s protocols. The proteins (25 μg) were loaded onto 7.5% to 15% SDS/PAGE gels, and then transferred to nitrocellulose membranes (Amersham Pharmacia Biotech), followed by blocking with 1% skim milk buffer overnight at 4 °C. Specifically, the Western blot for hepcidin was performed using a Mini-Protein TGX precast gel (Bio-Rad) and BioTrace NT membrane (PALL Gelman Laboratory). The primary antibodies against hepcidin and ferroportin were purchased from Abcam. Antibodies against IL-6 and β-actin were purchased from Santa Cruz Biotechnology and Sigma, respectively. The membranes were subsequently incubated with horseradish peroxidase-conjugated secondary antibody for 60 minutes at room temperature. Immunostaining with antibodies was performed with the Super Signal West Pico-enhanced chemiluminescence substrate (Thermo Scientific) and imaged with an AMERSHAM ImageQuant 800 (GE Healthcare Bio-Sciences). Quantification and normalization to the β-actin control were performed using ImageJ (version 1.48q).
- 5. Statistical analysis
- Statistical significance among the experimental groups was evaluated using the Mann-Whitney U test and the Kruskal-Wallis test for continuous variables, using the SPSS 18.0 software (IBM Corp). In all tables and images, data are presented as mean±standard deviation. A p-value less than 0.05 was considered statistically significant.
Methods
- 1. Baseline characteristics
- As shown in Table 1, 5/6 Nx rats exhibited the worst kidney function among the five groups. Among the 5/6 Nx groups, the hemoglobin levels were highest in the 5/6 Nx rats treated with cholecalciferol/omega-3 FA. Compared with the sham control group, 5/6 Nx rats showed significantly increased serum hepcidin levels and decreased serum vitamin D levels. After supplementation with either omega-3 FA or cholecalciferol, hepcidin levels decreased and vitamin D levels increased, with a concurrent improvement in anemia. Further, in 5/6 Nx rats treated with a combination of cholecalciferol and omega-3 FA, ferroportin and erythropoietin levels decreased, while iron and TIBC levels increased.
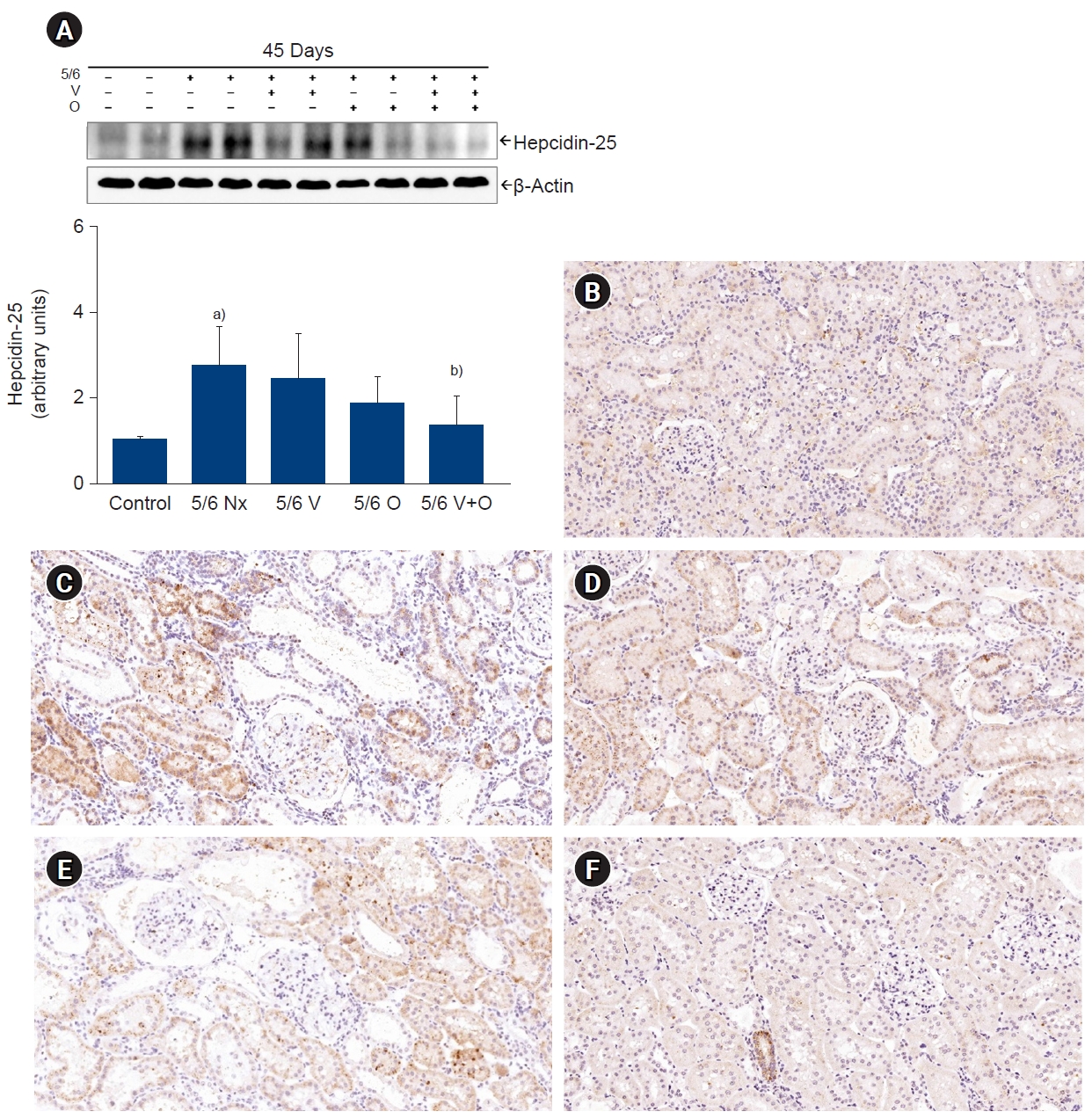
- 2. Hepcidin, ferroportin, and IL-6 expression in the kidney
- Hepcidin expression in the kidney was higher in 5/6 Nx rats than in controls. Interestingly, hepcidin expression was downregulated in 5/6 Nx rats following cholecalciferol/omega-3 FA supplementation (Fig. 1A).
- Immunohistochemistry staining of kidney sections showed that hepcidin was mainly expressed in the tubules of the sham controls (Fig. 1B-F). Conversely, its expression was markedly increased in the kidney of 5/6 Nx rats but decreased with the combined cholecalciferol and omega-3 FA treatment.
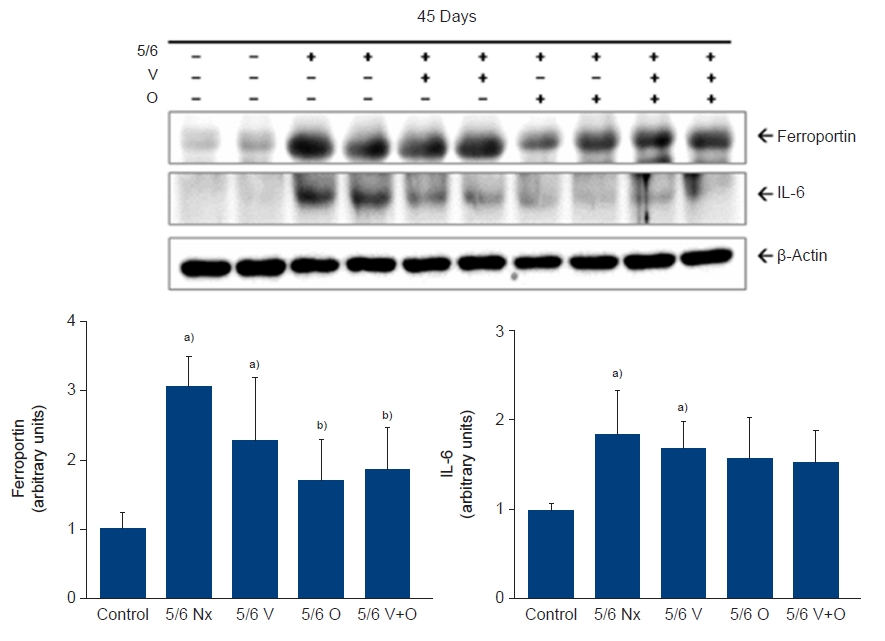
- Western blotting analysis revealed an upregulation of ferroportin expression in the kidney of 5/6 Nx rats compared with the controls (Fig. 2). Its expression was downregulated with either omega-3 FA monotherapy or following the combined cholecalciferol/omega-3 FA treatment. Moreover, IL-6 expression was increased in 5/6 Nx rats and a reverse trend was observed after the combined cholecalciferol/omega-3 FA supplementation (Fig. 2).
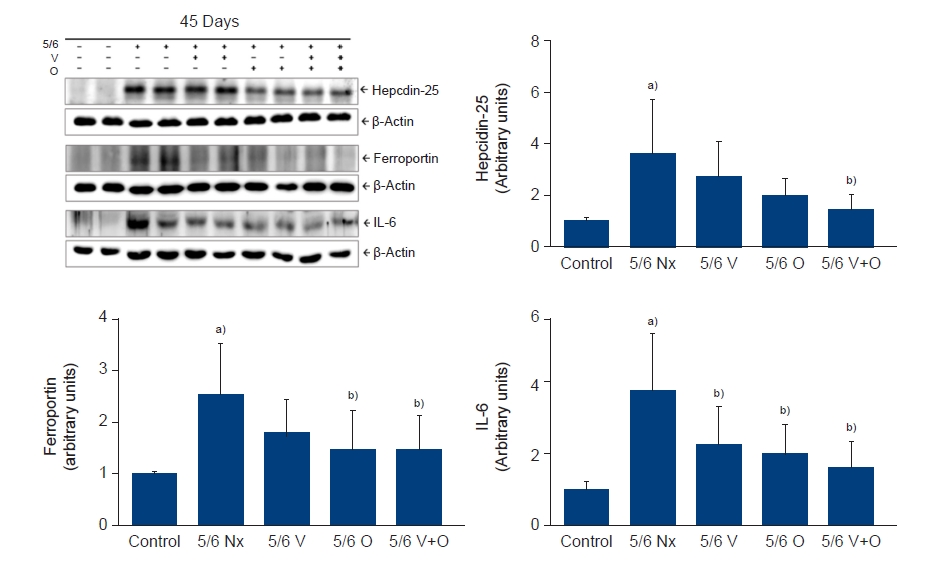
- 3. Hepcidin, ferroportin, and IL-6 expression in the kidney
- We observed the expression of hepcidin, ferroportin, and IL-6 in the liver of 5/6 Nx rats (Fig. 3). Compared with the sham control group, 5/6 Nx rats showed a significant upregulation of hepcidin expression. Supplementation of cholecalciferol/omega-3 FA led to a decrease in hepcidin levels. Ferroportin expression was higher in 5/6 Nx rats than in controls. Its expression was downregulated with omega-3 FA monotherapy or the combined cholecalciferol/omega-3 FA treatment. IL-6 expression was downregulated in 5/6 Nx rats following cholecalciferol/omega-3 FA supplementation. IL-6 expression was upregulated in 5/6 Nx rats compared with the controls and downregulated with cholecalciferol or omega-3 FA supplementation.
Results
- In this study, we found that both cholecalciferol and omega-3 FA supplementation improved hemoglobin levels in 5/6 Nx rats. Interestingly, the greatest effect was observed when cholecalciferol and omega-3 FA were administered together. The increase in hepcidin levels and the simultaneous decrease in TIBC and hemoglobin levels were significantly reversed by the combined cholecalciferol/omega-3 FA treatment. Our data showed that decreasing hepcidin levels by cholecalciferol and omega-3 FA may be a potential strategy in CKD-induced anemia. In the context of CKD, anemia is usually treated with erythropoiesis-stimulating agents (ESA), iron infusions, and blood transfusions; however, these treatments are often accompanied by adverse events. Therefore, safer and more effective treatment options for CKD-induced anemia are needed. In this study, we showed that the supplementation of cholecalciferol combined with omega-3 FA may be a viable strategy for decreasing hepcidin levels.
- Hepcidin is upregulated by inflammation, iron excess, and cancer [18], and downregulated in hypoxic conditions, iron deficiency, and enhanced erythropoiesis [19]. CKD is a chronic inflammatory state and hepatic hepcidin synthesis is associated with inflammation [20,21]. In patients with CKD, hepcidin levels are elevated due to decreased renal excretion or inflammation and increased expression due to excessive iron levels. Hepcidin is also involved in the ESA resistance mechanism, by reducing the release of iron from storage tissues or limiting iron availability for erythropoiesis. Vitamin D supplementation may inhibit the production of inflammatory cytokines [22]. Accordingly, we observed that the expression of IL-6 and ferritin, which is one of the increased inflammatory markers observed in 5/6 Nx rats, tends to reverse after supplementation with the combined cholecalciferol/omega-3 FA. IL-6 stimulates hepcidin synthesis via activation of the STAT3 pathway [23]. Therefore, vitamin D and omega-3 FA could reduce hepcidin levels in 5/6 Nx rats via an anti-inflammatory effect. It has been reported that the use of vitamin D and omega-3 FA monotherapy may lower hepcidin levels [13,24]. However, no studies to date have examined the combined effect of vitamin D and omega-3 FA on the hepcidin levels, but our study showed their synergic effect on hepcidin and hemoglobin levels. In this study, 50% of serum hepcidin levels were decreased in single omega-3 FA or cholecalciferol treated 5/6 Nx group without significant improvement of renal function compared to 5/6 Nx control group. Therefore, the improvement of serum hepcidin levels was not just by improvement of renal function. Although significant improvement of renal function by omega-3 FA and cholecalciferol supplementation affect the serum hepcidin levels, combined treatment with omega-3 FA and cholecalciferol may be beneficial for decreasing hepcidin levels and renal function in 5/6 Nx rat model. We observed an increase in the serum iron and TIBC levels and a decrease of hepcidin expression in rats treated with both cholecalciferol and omega-3 FA. Thus, we suspect that the reduction of serum hepcidin increases the efflux of iron from storage sites.
- Ferroportin is an iron exporter protein. Hepcidin binds to ferroportin, blocking the cellular iron exit. Low hepcidin levels are generally associated with high levels of ferroportin. However, the relationship between ferroportin and hepcidin is unclear. Unexpectedly, despite showing increased hepcidin levels, 5/6 Nx rats showed significantly elevated levels of ferroportin. In addition, increased erythropoietin and reduced hemoglobin and iron levels and increasing tendency ferritin levels were found in 5/6 Nx rats. On the contrary, decreased ferroportin and erythropoietin and increased hemoglobin and iron levels and decreasing tendency ferritin levels were found in 5/6 Nx rats supplemented with combined cholecalciferol/omega-3 FA. These finding may be explained by compensatory mechanism. Decreased hemoglobin levels may activate ferroportin expression and erythropoietin stimulation of remnant kidney and recovered hemoglobin levels by cholecalciferol/omega-3 FA may suppress ferroportin expression and erythropoietin stimulation of remnant kidney. In a previous study, increased expression of duodenal ferroportin was found in CKD rats [25,26]. Hepcidin expression was found in the kidney tubules as well as liver [27]. Further studies are needed to identify the exact mechanism according to hemoglobin levels and remnant renal function.
- Vitamin D insufficiency, as well as the presence of anemia, have been associated with resistance to ESA [8,10,28,29]. Recent studies shed light on the role of vitamin D in modulating the hepcidin levels [13,30]. In human hepatocytes and monocytes, vitamin D directly downregulates hepcidin expression by binding to vitamin D response elements in the hepcidin gene (HAMP) promoter [13]. In the same study, vitamin D repletion (in the ergocalciferol form) in a healthy cohort has been shown to decrease hepcidin levels with a concurrent increase of 25(OH)D levels [13]. In patients with stage 2-3 CKD, an inverse relationship between hepcidin and 25(OH)D levels was found [30]. In this study, the group treated with cholecalciferol showed no improvement in hepcidin and IL-6 levels compared with the group supplemented with additional omega-3 FA. The dramatic effect may be mediated via additional anti-inflammatory mechanisms and elevated 25(OH)D levels induced by additional omega-3 FA supplementation. Also, it was reported that high-dose vitamin D supplementation was associated with beneficial effects on erythropoiesis and iron availability in patients with low baseline vitamin D levels [31]. Further studies are needed to evaluate the effect of different doses of vitamin D on hepcidin levels.
- Our study utilized cholecalciferol rather than ergocalciferol supplementation. Another study showed that the treatment of patients with CKD using calcitriol showed no significant changes in the hepcidin levels [32]. Recent study reported that hepcidin levels slightly increased in the 3-day short term after cholecalciferol supplementation in patients with hemodialysis [33]. Although some studies reported that hepcidin levels decrease after cholecalciferol supplementation, the ability of vitamin D to regulate hepcidin levels and iron parameters in patients with CKD is debated. Further studies will be required to investigate the effect of different forms of vitamin D on hepcidin levels.
- Given the cost and adverse effects associated with escalating ESA therapy in patients with CKD, a treatment based on cholecalciferol and omega-3 FA would be an attractive adjuvant therapy to modulate the hepcidin levels.
- In conclusion, cholecalciferol and omega-3 FA are potent modulators of hepcidin levels and may be used in combination as a management strategy in anemia associated with low vitamin D and/or CKD. Further studies are needed to confirm the effect of cholecalciferol and omega-3 FA on the modulation of the hepcidin levels in patients with CKD.
Discussion
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
This study was supported by the National Research Foundation of Korea (2017R1C1B5016636).
-
Author contributions
Conceptualization: WSA, SML. Data curation: YIJ, HJJ, MHL, YKS, SEK, WSA, SML. Methodology: YIJ, HJJ, MHL, YKS, SEK, WSA, SML. Formal analysis: MHL, WSA, SML. Supervision: YIJ, HJJ, MHL, YKS, SEK, WSA, SML. Writing – original draft: YIJ, WSA, SML. Writing – review & editing: YIJ, WSA, SML. Approval of final manuscript: all authors.
Article information

| Variable | Control (n=6) | 5/6 Nx (n=6) | 5/6 Nx with cholecalciferol (n=6) | 5/6 Nx with omega-3 FA (n=6) | 5/6 Nx with cholecalciferol and omega-3 FA (n=6) | p-value |
|---|---|---|---|---|---|---|
| Final body weight (g) | 463.5±9.4 | 385.3±11.1a) | 419.8±32.8a) | 422.0±10.1a),b) | 421.7±12.2a),b) | <0.001 |
| Hemoglobin (g/dL) | 15.4±0.2 | 10.4±0.9a) | 11.2±1.2a) | 12.3±0.8a),b) | 13.3±0.6a),b),c) | <0.001 |
| Blood urea nitrogen (mg/dL) | 18.4±0.7 | 77.1±35.2a) | 72.3±22.9a) | 67.8±18.5 | 55.0±12.9b),c) | 0.003 |
| Creatinine (mg/dL) | 0.4±0.0 | 1.3±0.6a) | 1.2±0.3a) | 1.1±0.3 | 0.9±0.2b),c),d) | 0.002 |
| 25(OH)D (ng/mL) | 97.5±5.6 | 27.8±16.5a) | 50.4±41.7 | 61.6±38.5b) | 111.1±37.1b),c),d) | 0.003 |
| 1,25(OH)2D (pg/mL) | 170.9±40.5 | 44.6±16.9a) | 58.0±41.0a) | 83.1±42.3a) | 107.9±43.3a),b),c) | 0.002 |
| Hepcidin (ng/mL) | 2.0±0.5 | 12.1±11.4a) | 5.7±1.6a) | 5.8±2.6a) | 4.0±1.0a),b),c) | 0.005 |
| Erythropoietin (ng/mL) | 1.9±2.6 | 12.4±7.3a) | 11.4±11.8 | 8.8±16.4 | 3.4±7.8b),c) | 0.033 |
| Ferritin (μg/mL) | 1.3±0.4 | 2.4±3.0 | 1.2±0.5 | 1.1±0.3 | 1.3±0.3 | 0.505 |
| Ferroportin (ng/mL) | 1.1±0.2 | 1.8±0.5a) | 1.7±0.7 | 1.4±0.9 | 0.7±0.4b),c) | 0.008 |
| Iron (μg/dL) | 200.2±61.2 | 122.5±43.8a) | 119.3±45.1a) | 160.1±26.2a),c) | 154.3±11.8a),c) | 0.008 |
| UIBC (μg/dL) | 345.5±95.9 | 240.3±65.8a) | 283.8±106.0 | 250.9±120.7 | 318.0±47.8b) | 0.220 |
| TIBC (μg/dL) | 545.6±67.3 | 362.8±70.2a) | 403.1±94.6a) | 411.0±122.7a) | 472.3±45.8a),b) | 0.005 |
Values are presented as means±standard deviation.
Nx, nephrectomy; FA, fatty acid; 25(OH)D, 25-hydroxyvitamin D; 1,25(OH)2D, 1,25-dihydroxyvitamin D; UIBC, unsaturated iron-binding capacity; TIBC, total iron-binding capacity.
a) p<0.05, compared to the control group.
b) p<0.05, compared to the 5/6 Nx group.
c) p<0.05, compared to the 5/6 Nx with cholecalciferol group.
d) p<0.05, compared to the 5/6 Nx with omega-3 FA group.
- 1. Stauffer ME, Fan T. Prevalence of anemia in chronic kidney disease in the United States. PLoS One 2014;9:e84943.ArticlePubMedPMC
- 2. Levin A, Stevens PE, Bilous RW, Coresh J, De Francisco ALM, De Jong PE, et al. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 2013;3:1–150.Article
- 3. Finkelstein FO, Story K, Firanek C, Mendelssohn D, Barre P, Takano T, et al. Health-related quality of life and hemoglobin levels in chronic kidney disease patients. Clin J Am Soc Nephrol 2009;4:33–8.ArticlePubMedPMC
- 4. Spinowitz B, Pecoits-Filho R, Winkelmayer WC, Pergola PE, Rochette S, Thompson-Leduc P, et al. Economic and quality of life burden of anemia on patients with CKD on dialysis: a systematic review. J Med Econ 2019;22:593–604.ArticlePubMedPDF
- 5. Gouva C, Nikolopoulos P, Ioannidis JP, Siamopoulos KC. Treating anemia early in renal failure patients slows the decline of renal function: a randomized controlled trial. Kidney Int 2004;66:753–60.ArticlePubMed
- 6. Rao M, Pereira BJ. Optimal anemia management reduces cardiovascular morbidity, mortality, and costs in chronic kidney disease. Kidney Int 2005;68:1432–8.ArticlePubMed
- 7. National Kidney Foundation. KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for Anemia in Chronic Kidney Disease. Am J Kidney Dis 2006;47(5 Suppl 3):S11–145.ArticlePubMed
- 8. Kendrick J, Targher G, Smits G, Chonchol M. 25-Hydroxyvitamin D deficiency and inflammation and their association with hemoglobin levels in chronic kidney disease. Am J Nephrol 2009;30:64–72.ArticlePubMedPDF
- 9. Patel NM, Gutierrez OM, Andress DL, Coyne DW, Levin A, Wolf M. Vitamin D deficiency and anemia in early chronic kidney disease. Kidney Int 2010;77:715–20.ArticlePubMed
- 10. Kiss Z, Ambrus C, Almasi C, Berta K, Deak G, Horonyi P, et al. Serum 25(OH)-cholecalciferol concentration is associated with hemoglobin level and erythropoietin resistance in patients on maintenance hemodialysis. Nephron Clin Pract 2011;117:373–8.ArticlePubMedPDF
- 11. Nemeth E, Tuttle MS, Powelson J, Vaughn MB, Donovan A, Ward DM, et al. Hepcidin regulates cellular iron efflux by binding to ferroportin and inducing its internalization. Science 2004;306:2090–3.ArticlePubMed
- 12. Mercadal L, Metzger M, Haymann JP, Thervet E, Boffa JJ, Flamant M, et al. The relation of hepcidin to iron disorders, inflammation and hemoglobin in chronic kidney disease. PLoS One 2014;9:e99781.ArticlePubMedPMC
- 13. Bacchetta J, Zaritsky JJ, Sea JL, Chun RF, Lisse TS, Zavala K, et al. Suppression of iron-regulatory hepcidin by vitamin D. J Am Soc Nephrol 2014;25:564–72.ArticlePubMed
- 14. An WS, Lee SM, Son YK, Kim SE, Kim KH, Han JY, et al. Effect of omega-3 fatty acids on the modification of erythrocyte membrane fatty acid content including oleic acid in peritoneal dialysis patients. Prostaglandins Leukot Essent Fatty Acids 2012;86:29–34.ArticlePubMed
- 15. Sidiartha IG, Bakta IM, Wiryana IM, Sutirtayasa IW, Sjarif DR. Eicosapentaenoic acid and docosahexaenoic acid in fish oil capsule supplementation in obese children decreases serum interleukin-6 and hepcidin and improves iron status. Bali Med J 2017;6:97–101.Article
- 16. Lee SM, Lee MH, Son YK, Kim SE, An WS. Combined treatment with omega-3 fatty acid and cholecalciferol increases 1,25-dihydroxyvitamin d levels by modulating dysregulation of vitamin D metabolism in 5/6 nephrectomy rats. Nutrients 2019;11:2903.ArticlePubMedPMC
- 17. An WS, Kim HJ, Cho KH, Vaziri ND. Omega-3 fatty acid supplementation attenuates oxidative stress, inflammation, and tubulointerstitial fibrosis in the remnant kidney. Am J Physiol Renal Physiol 2009;297:F895–903.ArticlePubMed
- 18. Schmidt PJ. Regulation of iron metabolism by hepcidin under conditions of inflammation. J Biol Chem 2015;290:18975–83.ArticlePubMedPMC
- 19. Ashby DR, Gale DP, Busbridge M, Murphy KG, Duncan ND, Cairns TD, et al. Erythropoietin administration in humans causes a marked and prolonged reduction in circulating hepcidin. Haematologica 2010;95:505–8.ArticlePubMed
- 20. Yilmaz MI, Solak Y, Covic A, Goldsmith D, Kanbay M. Renal anemia of inflammation: the name is self-explanatory. Blood Purif 2011;32:220–5.ArticlePubMedPDF
- 21. Bowry SK, Gatti E. Impact of hemodialysis therapy on anemia of chronic kidney disease: the potential mechanisms. Blood Purif 2011;32:210–9.ArticlePubMedPDF
- 22. Calton EK, Keane KN, Newsholme P, Soares MJ. The impact of vitamin D levels on inflammatory status: a systematic review of immune cell studies. PLoS One 2015;10:e0141770.ArticlePubMedPMC
- 23. Verga Falzacappa MV, Vujic Spasic M, Kessler R, Stolte J, Hentze MW, Muckenthaler MU. STAT3 mediates hepatic hepcidin expression and its inflammatory stimulation. Blood 2007;109:353–8.ArticlePubMedPDF
- 24. Tabibi H, Mirfatahi M, Hedayati M, Nasrollahi A. Effects of flaxseed oil on blood hepcidin and hematologic factors in hemodialysis patients. Hemodial Int 2017;21:549–56.ArticlePubMedPDF
- 25. Garrido P, Ribeiro S, Fernandes J, Vala H, Bronze-da-Rocha E, Rocha-Pereira P, et al. Iron-hepcidin dysmetabolism, anemia and renal hypoxia, inflammation and fibrosis in the remnant kidney rat model. PLoS One 2015;10:e0124048.ArticlePubMedPMC
- 26. Hamada Y, Kono TN, Moriguchi Y, Higuchi M, Fukagawa M. Alteration of mRNA expression of molecules related to iron metabolism in adenine-induced renal failure rats: a possible mechanism of iron deficiency in chronic kidney disease patients on treatment. Nephrol Dial Transplant 2008;23:1886–91.ArticlePubMed
- 27. van Swelm RP, Wetzels JF, Verweij VG, Laarakkers CM, Pertijs JC, van der Wijst J, et al. Renal handling of circulating and renal-synthesized hepcidin and its protective effects against hemoglobin-mediated kidney injury. J Am Soc Nephrol 2016;27:2720–32.ArticlePubMedPMC
- 28. Lac PT, Choi K, Liu IA, Meguerditchian S, Rasgon SA, Sim JJ. The effects of changing vitamin D levels on anemia in chronic kidney disease patients: a retrospective cohort review. Clin Nephrol 2010;74:25–32.ArticlePubMed
- 29. Icardi A, Paoletti E, De Nicola L, Mazzaferro S, Russo R, Cozzolino M. Renal anaemia and EPO hyporesponsiveness associated with vitamin D deficiency: the potential role of inflammation. Nephrol Dial Transplant 2013;28:1672–9.ArticlePubMed
- 30. Zughaier SM, Alvarez JA, Sloan JH, Konrad RJ, Tangpricha V. The role of vitamin D in regulating the iron-hepcidin-ferroportin axis in monocytes. J Clin Transl Endocrinol 2014;1:19–25.ArticlePubMed
- 31. Pistis KD, Westerberg PA, Qureshi AR, Beshara S, Sterner G, Barany P, et al. The effect of high-dose vitamin D supplementation on hepcidin-25 and erythropoiesis in patients with chronic kidney disease. BMC Nephrol 2023;24:20.ArticlePubMedPMCPDF
- 32. Panwar B, McCann D, Olbina G, Westerman M, Gutierrez OM. Effect of calcitriol on serum hepcidin in individuals with chronic kidney disease: a randomized controlled trial. BMC Nephrol 2018;19:35.ArticlePubMedPMCPDF
- 33. Obi Y, Yamaguchi S, Hamano T, Sakaguchi Y, Shimomura A, Namba-Hamano T, et al. Effect of cholecalciferol on serum hepcidin and parameters of anaemia and CKD-MBD among haemodialysis patients: a randomized clinical trial. Sci Rep 2020;10:15500.ArticlePubMedPMCPDF
 PubReader
PubReader ePub Link
ePub Link Cite
Cite