Case Report of Prostate Cancer Patient with Only Lymph Node Involvement on F-18 FDG PET/CT
Article information
Abstract
We report a case of a patient with locally advanced prostate cancer who had only lymph node involvement without bone metastasis on F-18 FDG PET/CT.
A 62-year-old Korean male was admitted to our hospital due to dysuria. His PSA level on admission was 79.35 ng/mL. A transrectal ultrasound-guided prostate biopsy confirmed prostate cancer and his Gleason score was 10 (5+5). F-18 FDG PET/CT demonstrated a hypermetabolic mass lesion with SUVmax 7.0 in the prostate and hypermetabolism with SUVmax 4.7 of the abdominal and pelvic lymph nodes. Tc-99m HDP bone scan showed no significant bone metastasis. The patient underwent hormonal therapy for 9 months. Follow-up F-18 FDG PET/CT showed significantly reduced size and FDG uptake in the prostate and abdominal and pelvic lymph nodes. In this case, treatment monitoring with F-18 FDG PET/CT showed decreased mass size and FDG uptake in the prostate and abdominal and pelvic lymph nodes.
Prostate cancer is a slowly growing cancer that is asymptomatic and presents a high risk of metastasis. Although patients with localized prostate cancer often receive curative treatment, many will eventually develop recurrence and metastasis.1 F-18 fluorodeoxyglucose positron emission tomography/computed tomography (PET/CT) is employed for diagnosis, staging, monitoring of treatment response, surveillance and for predicting prognosis in a variety of cancers, leading to improved management in many patients.234 A previous study reported that PET/CT may be useful for diagnosing and staging high Gleason score patients for primary prostate cancer tumors, for detecting locally recurrent and/or metastatic disease in patients with increasing prostate specific antigen (PSA) level, for monitoring therapy, and for predicting prognosis.5 In this paper, we report the case of a locally advanced prostate cancer patient who had only lymph node involvement on PET/CT conducted for diagnosis and treatment monitoring.
CASE
A 62-year-old Korean male was admitted to our hospital due to dysuria. His PSA level on admission was 79.35 ng/mL. A transrectal ultrasound-guided prostate biopsy confirmed prostate cancer and his Gleason score was 10 (5+5). Contrast-enhanced abdominal CT scan showed a 7.0 cm multilobulated mass in the prostate with direct invasion of the urinary bladder and rectum along with enlargement of multiple lymph nodes in the abdominal paraaortic, both iliac, and inguinal areas. Tc-99m hydroxymethylene diphosphonate bone scintigraphy showed no significant focal tracer uptake indicative of bone metastasis (Fig. 1). PET/CT was performed to screen for other malignant diseases and showed a mass lesion with FDG uptake with a maximum standardized uptake value (SUVmax) of 4.6 in the prostate (Fig. 2a) along with lymph node enlargement with FDG uptake of SUVmax 3.4 in the paraaortic (Fig. 2b), both iliac, and inguinal areas. The patient underwent hormonal therapy for 9 months. His follow-up PSA level after hormonal therapy was decreased (5.74 ng/mL) and follow-up PET/CT showed significantly reduced size and FDG uptake in the prostate and abdominal and pelvic lymph nodes (Fig. 2c,d).

A 62-year-old male underwent Tc-99m HDP bone scintigraphy for searching bone metastasis. Tc-99m HDP bone scintigraphy showed multiple tracer uptake in the wrist, knee, ankle and hand joints, associated with arthritis, but no significant focal tracer uptake of bone metastasis.
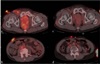
F-18 FDG PET/CT showed a mass lesion with FDG uptake with SUVmax 4.6 in the prostate (a) and lymph node enlargement with FDG uptake with SUVmax 3.4 in paraaortic (b) areas. Follow-up F-18 FDG PET/CT about 9 months after hormonal therapy showed a significantly reduced size and FDG uptake in the prost
DISCUSSION
Prostatic adenocarcinoma is associated with high risk of metastasis. The most frequent location is the bones, where more than 90% of long-term metastasis occurs.6 Several other locations have been reported including the small intestine (1 – 4%) and the cecum, but never the rectum.7 Some autopsy series revealed that 9% of patients who presented with prostate adenocarcinoma had contiguity invasion of the rectum.8 The growth and dissemination patterns of prostate cancer are well known. Involvement of the prostatic capsule, bladder base, and seminal vesicles can occur via direct extension, whereas the invasion of pelvic and abdominal lymph nodes can occur via lymphatic dissemination. Hematogenous spread most often manifests to the bone, lung and liver.9 In this paper, we describe a rare case limited to lymph nodes metastases detected by PET/CT in a patient with prostate cancer.
Early studies of PET/CT in prostate cancer showed that FDG accumulation in the primary prostate cancer is generally low, and may overlap with uptake in benign prostatic hyperplasia (BPH) and in the normal gland.10 Moreover, because the local extent of the tumor cannot be accurately assessed, PET/CT has limited utility in the staging of disease at the time of initial diagnosis.11 However, Jadvar et al. reported that F-18 FDG PET clearly localized nodal metastatic disease, while CT demonstrates non-diagnostic subcentimeter lymph nodes.12 Other studies also reported that PET/CT may be useful in the evaluation of patients with advanced disease and higher Gleason grades and serum PSA levels for the detection of active osseous and soft tissue metastases as well as in the evaluation of hormonal treatment response.131415 The higher FDG uptake observed in this setting may be due to the faster rate of tumor growth in comparison to slow growing or dormant tumors with lower Gleason scores. In our case, PET/CT revealed lymph node involvement and good therapeutic response, along with cessation of metabolism of the prostate cancer mass and multiple lymph node metastases.
In this unusual case of prostate cancer, we emphasize that using PET/CT for treatment monitoring showed decreased mass size and FDG uptake in the prostate and abdominal and pelvic lymph nodes. PET/CT is helpful in the diagnosis and treatment monitoring of prostate cancer limited to the lymph nodes.