Usefulness of Kaloderm® in Finger Tip Necrosis : A Case Report
Article information
Abstract
We experienced a case of crush injury of the hand for which we performed a flap surgery and treated the necrotic parts placement using cultured allogeneic keratinocytes (Kaloderm®) with good results.
The patient was a 31-year-old woman whose left middle finger was caught in a door, causing a crush injury. Although primary repair was performed, a 2 × 2.5-cm-sized necrosis developed, and a V-Y advancement flap was performed after the removal of dead tissues. However, a 1 × 2-cm-sized partial necrosis occurred and was treated using Kaloderm®.
After the use of Kaloderm®, the patient’s wound was healed, and no complications, except for mild pain, were observed for 1 year after the surgery.
If a necrotic site appears after flap placement of fingertip, its treatment is difficult. If used well, Kaloderm® may be a good option for necrosis of the fingertips and other areas that are difficult to cure.
Soft tissue damage of the fingertips is frequently observed clinically, and crushed or peeling damage is especially common. Fingertip plays a crucial role in maintaining sensory and physical functions in such cases. The purpose of fingertip treatment is reconstructing the damaged distal end with soft tissue that has normal sensation and function, without pain.1
There have been tremendous advancements in dressing materials for postsurgical treatment. One such example is Kaloderm® (TEGO science, Seoul, Korea), which has been developed and used as allogeneic keratinocyte therapy. Kaloderm ® is known to promote healing by producing and secreting cytokines and growth factors when applied to wounds.2,3
In the present case, a V-Y advancement flap was performed on a patient with a crush injury on the left middle finger, and Kaloderm® was applied to the surgical site due to necrosis. Herein, we report the results of this case along with a literature review.
CASE
A 31-year-old female patient was admitted to the emergency room after suffering a crush injury when her left middle finger got stuck in a door. There was no remarkable medical history at the time of visit, and a deep laceration of about 2 cm was observed on the left middle finger. After the wound was sutured, necrosis of the wound gradually progressed during outpatient treatment, and a crust of about 2 × 2.5 cm was formed (Fig. 1). The patient complained of severe pain upon touch. A surgery to remove the necrosed tissue was performed 1 week following the suture. The necrosed region was mostly comprised of subcutaneous fat, and the bone was not exposed. A flap was performed in a V-Y pattern. Nevertheless, necrosis of approximately 1 × 2 cm reoccurred on the fingertip 2 days after surgery (Fig. 2). As most of the necrosis occurred in the region under the fingernail, it was difficult to perform secondary surgery. Based on the judgement that using allogeneic keratinocytes would be effective in treating this case, Kaloderm® was applied at regular intervals of 2–3 days for 2 weeks, and progress was observed. Two weeks following the flap, epithelialization progressed notably; the patient fully recovered and was discharged a week later. About 1 year later, the patient was once again admitted to the outpatient clinic, and she had normal sensation, as well as a satisfactory aesthetic outcome were observed (Fig. 3). Result of 2-point discrimination test was about 4mm. The patient aesthetic satisfaction score was 9 out of 10. She was very satisfied of left middle finger scar. But, she complained of intermittent pain. Pain in the fingertip notably improved following nerve block in cooperation with the Department of Anesthesiology and Pain Medicine. One year following the surgery, no complications were observed. A written consent was obtained from the patient for the publication of this case.
Preoperative view.

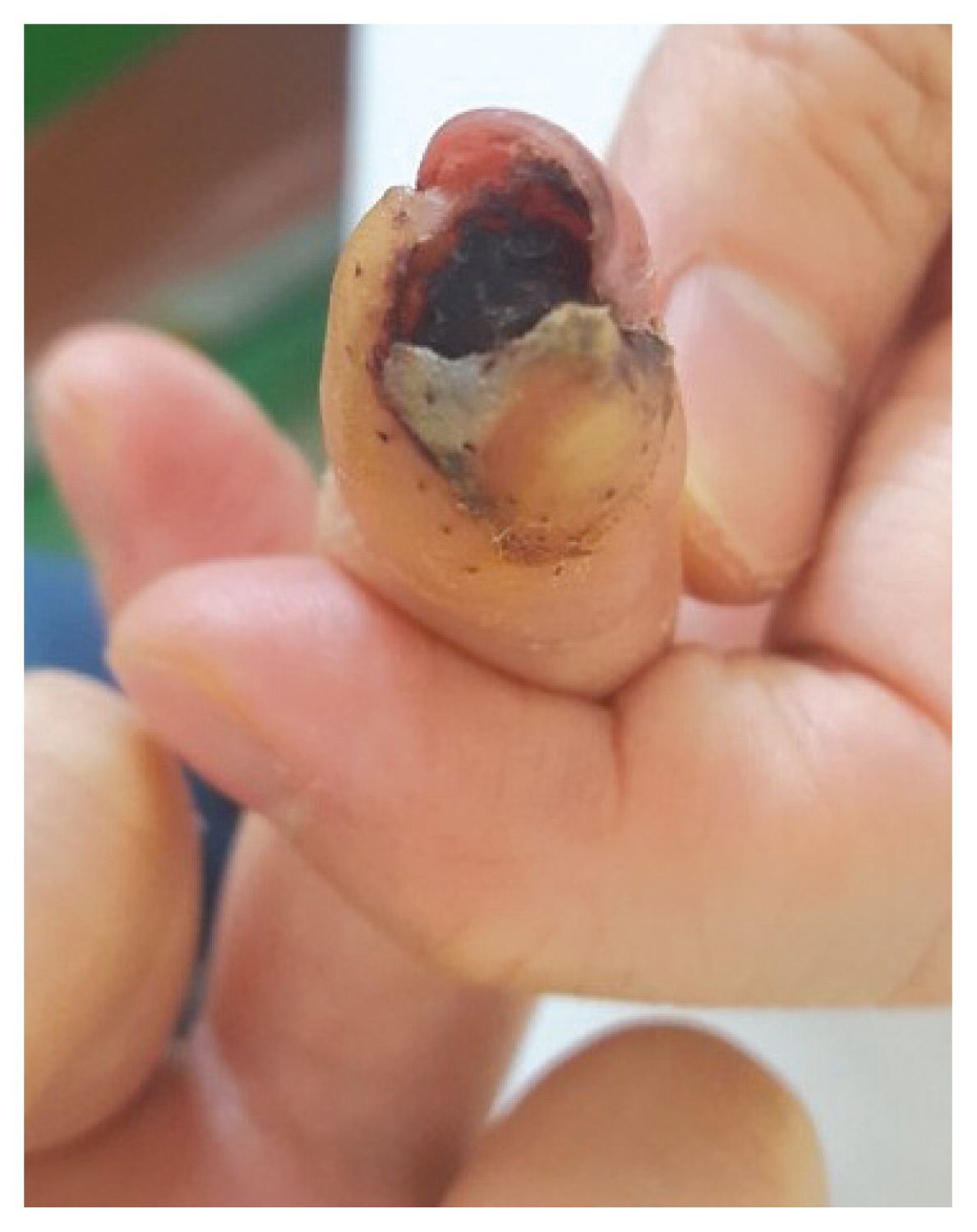
Patient’s photograph 2 days after V-Y advancement flap.

Postoperative photograph at 1 year follow-up, no significant complications were observed.
DISCUSSION
Damage to the fingertips is commonly encountered in clinics, and methods that can be used for reconstruction in these cases involve grafting, local flaps, and free flaps.4 Alternative surgical treatments can be primarily considered in case of necrosis following surgery, but recently, dressing materials have been developed and used as a treatment option.
Biological dressings that stimulate wound healing by delivering cytokines and growth factors locally have been developed and demonstrated positive results.5 Although not evidently verified thus far, it has been suggested that the induction of interleukin(IL)-1α, IL-β, IL-3, IL-6, and transforming growth factor α (TGF-α), as well as the extracellular matrix elements found in Kaloderm® promote epithelialization of the affected area.2–5 Many studies have reported the effects of allogeneic keratinocytes such as Kaloderm® on skin damage caused by diabetic foot ulcers, trauma, necrotizing fasciitis, and burns.6 Joo et al.7 stated that early resection of the necrosed tissue and Kaloderm® application accelerated epithelialization and shortened the healing time for deep burns in infants and reported more aesthetically satisfactory outcomes.
In the present case, necrosis progressed despite suturing the laceration from crush injury. Partial necrosis progressed once again after surgical removal of the necrosed tissue, despite performing a V-Y advancement flap. A secondary surgery was difficult due to the location of necrosis directly underneath the fingernail. Once Kaloderm® was applied over and over to the area, quick healing and positive aesthetic outcomes were achieved. If applications on fingertip skin damage that requires a graft are considered, the allogeneic keratinocyte may be used without surgical treatment, eliminating the occurrence of donor site scarring.
In conclusion, if a necrotic site appears after flap placement of fingertip, its treatment is difficult. If used well, Kaloderm® may be a good option for necrosis of the fingertips and other areas that are difficult to cure.