Tricuspid and pulmonary valve endocarditis associated with double-chambered right ventricle
Article information
Abstract
Abstract
We report a rare case of tricuspid valve and pulmonary valve endocarditis associated with a double-chambered right ventricle in an adult female with pulmonary artery aneurysm and septic pulmonary embolism by Streptococcus mitis. She was treated with aggressive antibiotic therapy followed by debridement of the infective lesion of tricuspid valve, pulmonary valve replacement using xenograft and resection of obstructing muscular bundles in right ventricle.
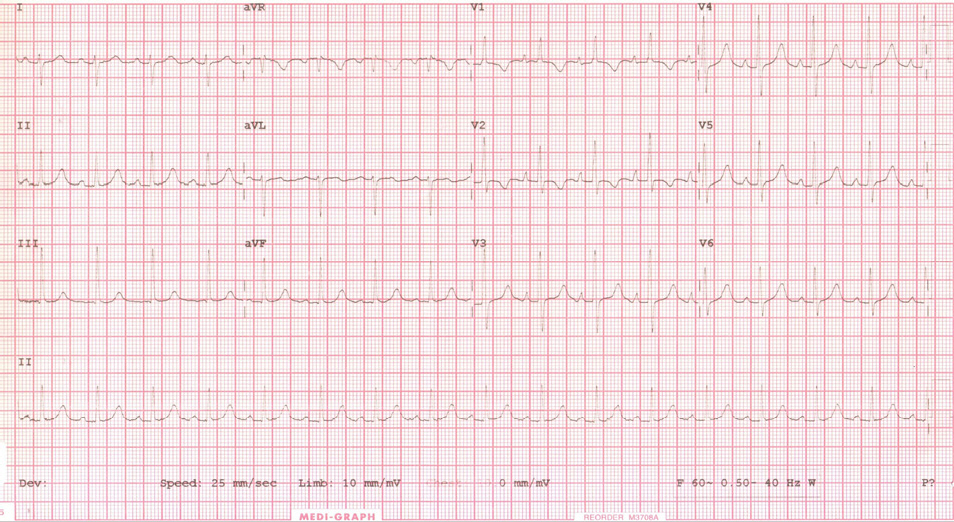
Initial electrocardiogram showing right ventricular hypertrophy with strain pattern, right axis deviation, and right atrial enlargement.

Pulmonary angio CT showing mild cardiomegaly with right heart enlargement and multiple distal pulmonary infarction (white arrow heads) with multiple pulmonary artery aneurysm (white arrows).

Transthoracic echocardiogram showing (A) continuous-wave Doppler tracing along the right ventricular outflow tract with peak gradient of 87 mmHg across the subinfundibulum (B) hypertrophied muscular bands dividing the right ventricle (white arrow) with D-shaped interventricular septum and large vegetation on pulmonary valve. LV: left ventricle, PV: pulmonary valve, RV: right ventricle.

Transesophageal echocardiogram showing echogenic shaggy materials (white arrow) on hypertrophied muscular bands, suspicious vegetations.