Complication of Amebic Liver Abscess: Biliary Fistula
Article information
Abstract
Abstract
In amebic liver abscess, communication between liver abscess and intrahepatic bile ducts is an uncommon cause of bile leak. This condition can be treated surgically or endoscopically. However, these treatment modalities are related with high morbidity and mortality. A 49-year-old man was diagnosed with amebic liver abscess. Percutaneous drainage was performed due to poor medical response and for the purpose of preventing abscess rupture. Liver abscess-biliary communication was found at follow-up imaging study. He was treated successfully with medical therapy and supportive care without further interventions.

(A) More than 12.3cm sized multilayered enhanced single lesion in right liver. (B) Markedly decreased size of hepatic abscess (10.7 -> 5.6cm) after PCD insertion, and even smaller fluid component.
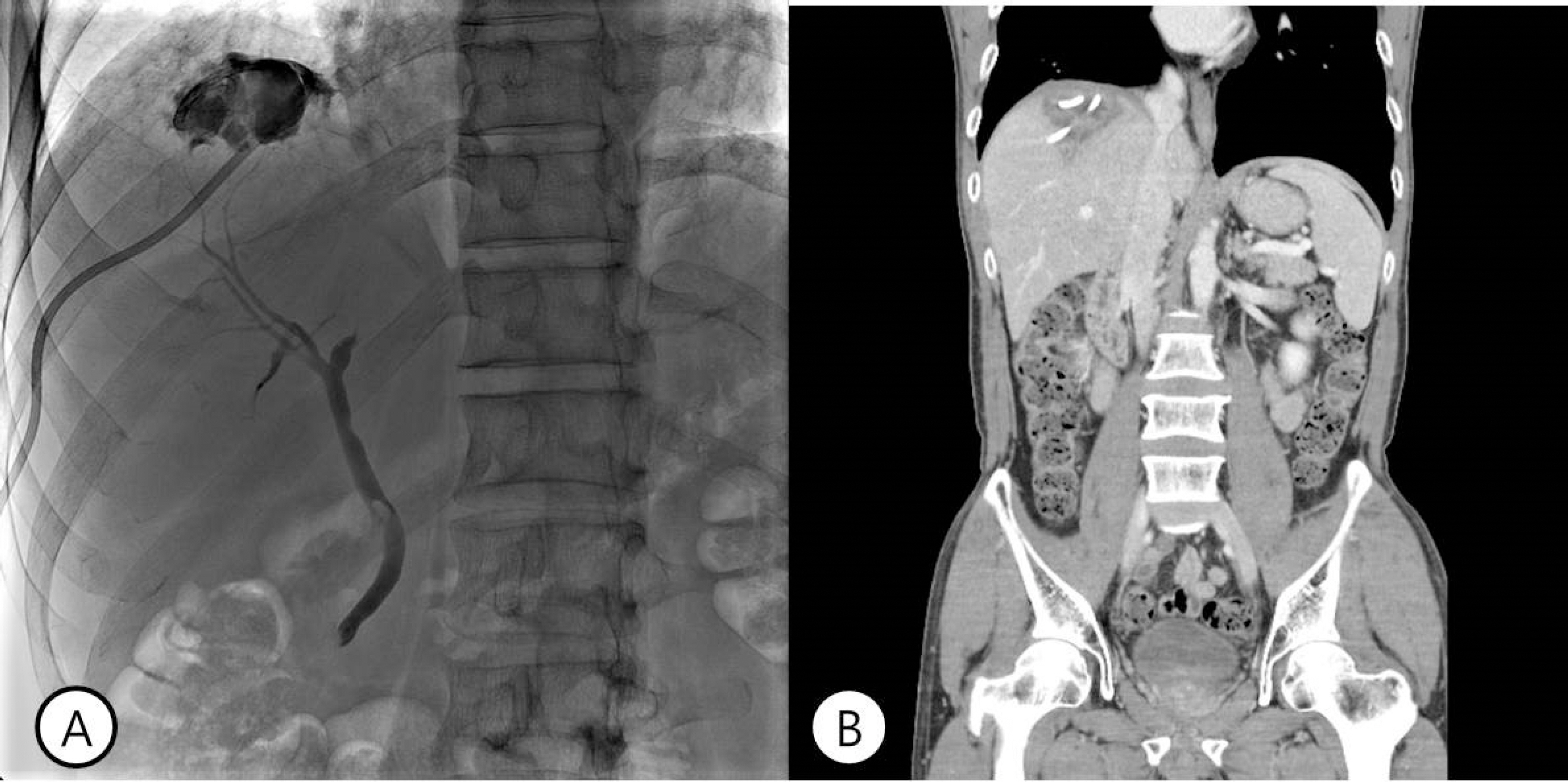
(A) Tubography showed abscess communicating with bile duct. Revealing a abscess-bile duct fistula at hospital day #22. (B) Minimally decreased size of hepatic abscess (5.6->5.4 cm) at hospital day #31.
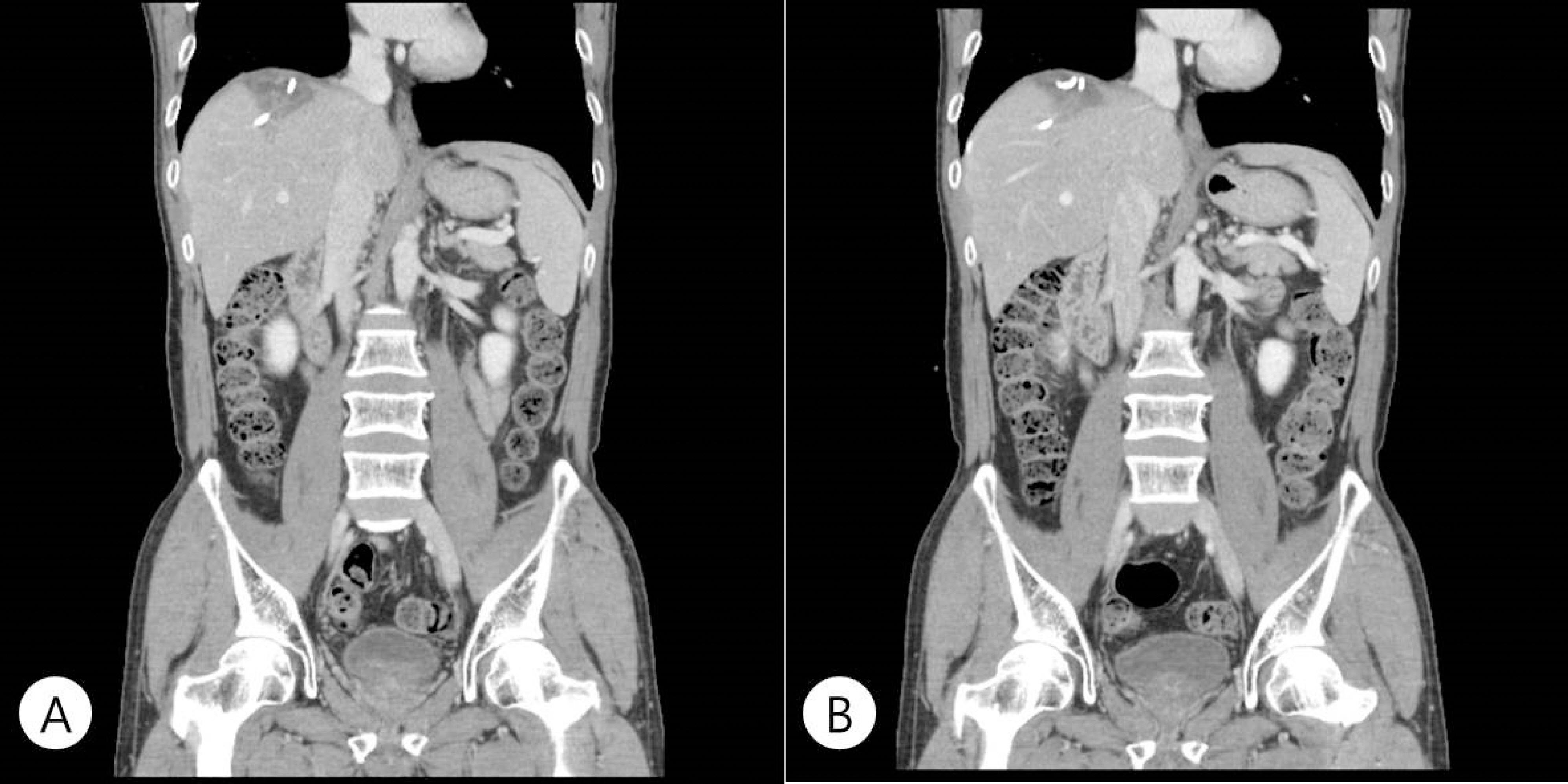
(A) Interval decreased abscess size (5.4->4.6 cm) and fluid content. Probably remained communication between biliary tract and abscess at hospital day #53. (B) Interval more decreased size of abscess in Rt liver dome (4.6 -> 4.2cm). Probably disappeared communication between biliary tract with abscess.

No connection into bile duct or hepatic vein. Removal of PCD tube at hospital day #67.