Polycystic Ovary Syndrome
Article information
Abstract
Abstract
Polycystic ovary syndrome affects 6%-7% of reproductive-aged women, making it the most common endocrine disorder in this population. It is characterized by chronic anovulation and hyperandrogenism. Affected women may present with reproductive manifestations such as irregular menses or infertility, or cutaneous manifestations, including hirsutism, acne, or male-pattern hair loss. Over the past decade, several serious metabolic complications also have been associated with polycystic ovary syndrome including type 2 diabetes mellitus, metabolic syndrome, sleep apnea, and possibly cardiovascular disease and nonalcoholic fatty liver disease. In addition to treating symptoms by regulating menstrual cycles and improving hyperandrogenism, it is imperative that clinicians recognize and treat metabolic complications. Lifestyle therapies are first-line treatment in women with polycystic ovary syndrome, particularly if they are overweight. Pharmacological therapies are also available and should be tailored on an individual basis. This article reviews the diagnosis, clinical manifestations, metabolic complications, and treatment of the syndrome.
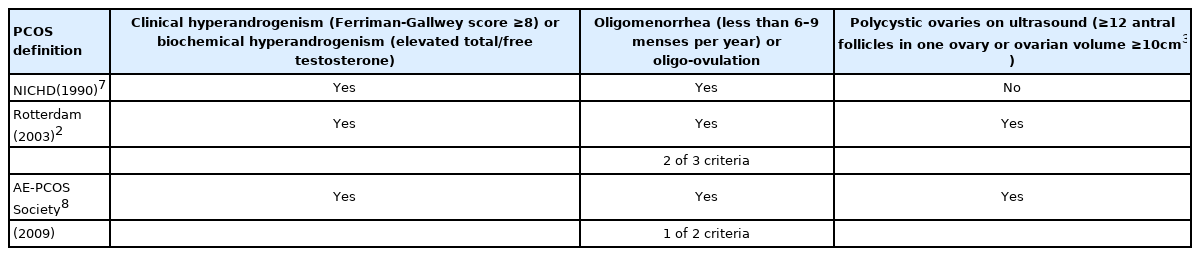
PCOS definitions 1990–20093

Posssible pathogenesis of polycystic ovary syndrome4

Laboratory testing to evaluate for metabolic complications of polycystic ovary syndrome1
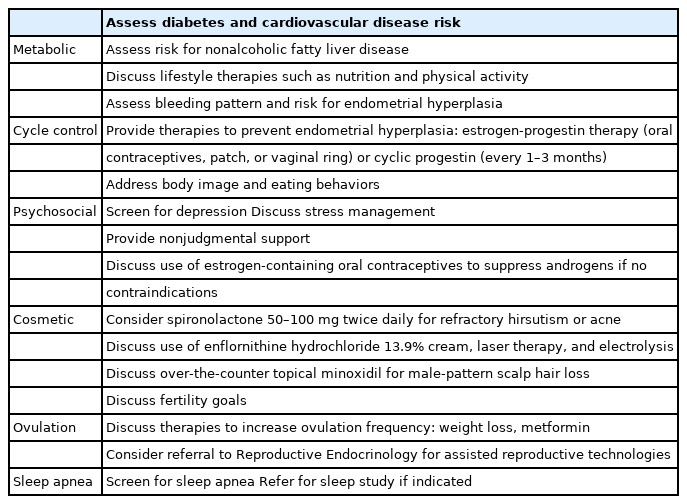
Summary of recommendations for addressing reproductive, cosmetic, metabolic, and psychological complications of polycystic ovary syndrome1