A Case of Adult onset Bartter Syndrome with Nephrocalcinosis
Article information
Abstract
Abstract
Bartter syndrome is a renal tubular defect in electrolyte transport characterized by hypokalemia, metabolic alkalosis, hyperreninemia, hyperaldosteronism, normal blood pressure, and other clinical symptoms. As a clinical and genetical heterogeneous disorder, this syndrome can be classified into two clinical variants, antenatal Bartter syndrome and classic Bartter syndrome according to the onset age. Nephrocalcinosis is common in antenatal Bartter syndrome, but is rare in classic Bartter syndrome. It can also be classified into five genetic subtypes by the underlying mutant gene, all of which are expressed in the tubular epithelial cells of the thick ascending limb of the loop of Henle. Patients with Bartter syndrome type 1, 2 and 4 present at a younger age than classic Bartter syndrome type 3. We have experienced a case of Bartter syndrome with nephrocalcinosis in a 42-year-old woman diagnosed by biochemical and radiologic studies. We had successful response with potassium chloride and spironolactone.

Renal Ultrasonography: Decreased kidney size with increased echogenicity of both renal medulla. This is a typical finding of medullary nephrocalcinosis.
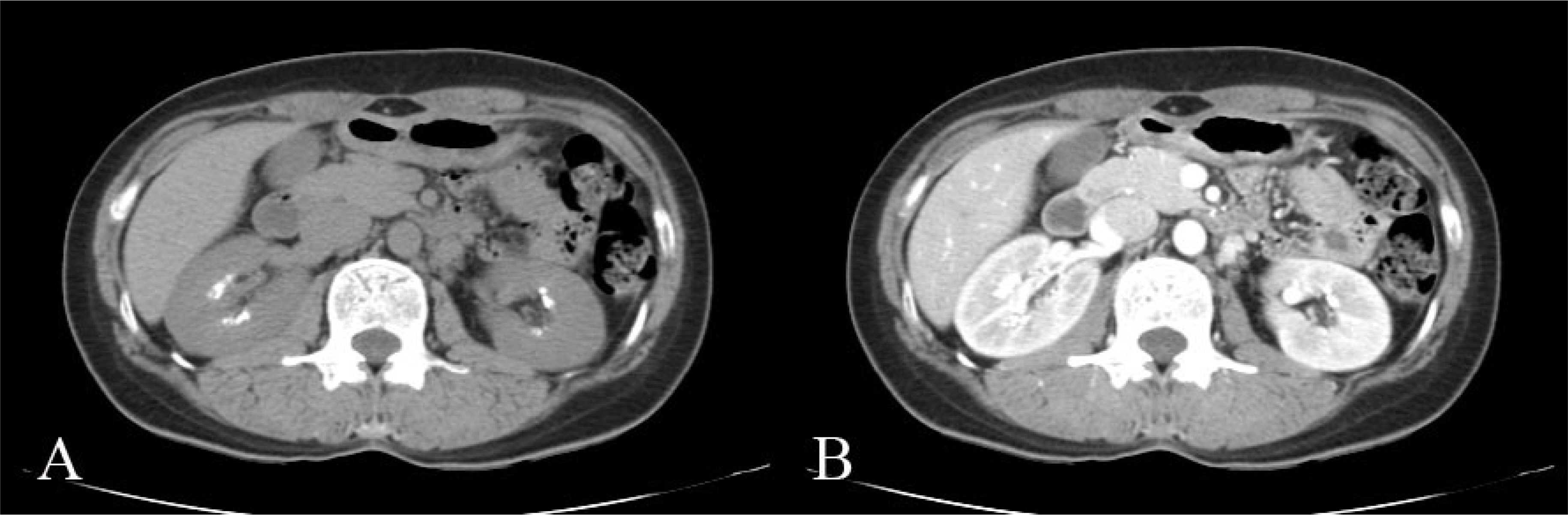
Abdominal CT : Bilateral calcifications clustered in the region of the renal medulla. (A) Pre-contrast enhanced image, (B) Contrast enhanced image.

Change of serum K levels before and after adding spironolactone to potassium chloride. tx=treatment, f/u= followup.