A Case of Oliguric Mannitol Induced Acute Kidney Injury Early Treated by Continuous Renal Replacement Therapy
Article information
Abstract
Abstract
We report oliguric mannitol-induced acute kidney injury (AKI) early treated by continuous renal replacement therapy. A 70-year-old woman was admitted to the Department of Neurology with diagnosis of acute intracranial hemorrhage. Mannitol was infused for intracranial pressure control. At admission third day, urine output was abruptly decreased to 57 ml during first 6 hours and blood urea nitrogen (BUN) and serum creatinine was increased to 54.2 mg/dL and 5.3 mg/dL respectively. Plasma osmolality was 340 mOsm/kg and osmolar gap was 70. Mannitol was immediately withdrawn and continuous renal replacement therapy (CRRT) was performed to remove mannitol rapidly. Urine output was increased 6 hours later after continuous veno-veno hemodiafiltration (CVVHDF) start. BUN and creatinine was decreased to 21.4 and 1.2 mg/dL at admission ninth day. Mannitol can develop oliguric AKI and CRRT may be of more benefit than conventional hemodialysis in the case of increased intracranial pressure.

Brain CT shows hemorrhage in thalamus extending into ventricle.
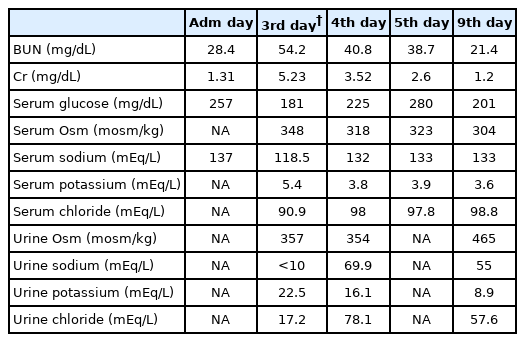
Changes of serum laboratory findings during admission