Efficacy of Foreign Body Removal using a Cryoprobe in Flexible Bronchoscopy
Article information
Abstract
Abstract
Objectives
Endobronchial foreign body impaction is a medical emergency because of the air way obstruction. Therefore, immediate foreign body removal is crucial in such situations. Recently, there have been several reports about cryoprobe use as a tool for removal of foreign bodies. In this study, we determined the efficacy and complications of foreign body removal using a cryoprobe during flexible bronchoscopy.
Methods
This is a retrospective review of 27 patients who visited Kosin University Gospel Hospital from August 2007 to August 2010 with respiratory symptoms due to a foreign body in the airway. There were 17 males and 10 females, aged from 7 to 78 years. The foreign bodies were more frequently located (55%) in the right bronchus. The cryoprobe was inserted through the forceps channel of the flexible bronchoscope under local anesthesia. The lesion was quickly frozen for 5 seconds at -80℃, and the bronchoscope was removed with the probe after crystal formation on the contacted area.
Results
The success rate of removal of foreign bodies was 85% (23/27) using the cryoprobe. One case of broncholith did not undergo attempted removal because of the possibility of excessive hemorrhage by the tight bronchus impaction, and three cases (plastic, silicon, and implant) failed due to limited crystal formation. There were no severe hemorrhages, arrhythmias, or casualties during the procedure.
Conclusions
The removal of foreign body using a cryoprobe during flexible bronchoscopy was shown to be safe and effective. The nature of the material should be attempted before removing a foreign body.
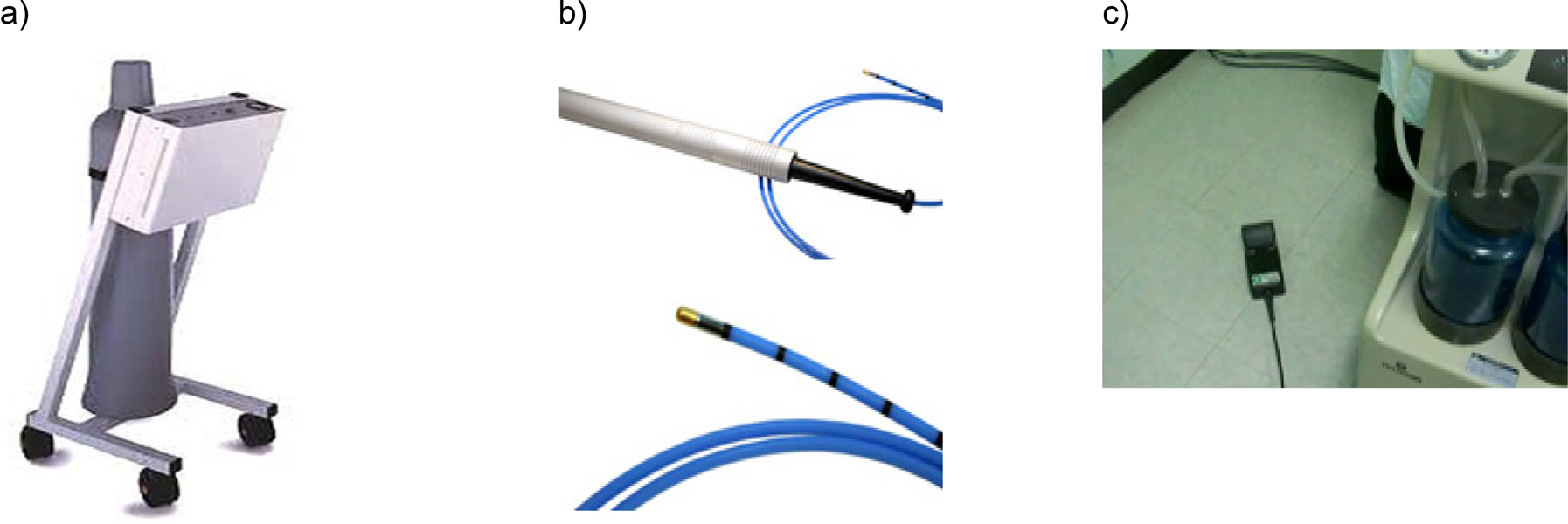
The system for cryoprobe removal, a) cryosurgical unit b) flexible cryoprobe and c)pedal of the cryosurgical unit.
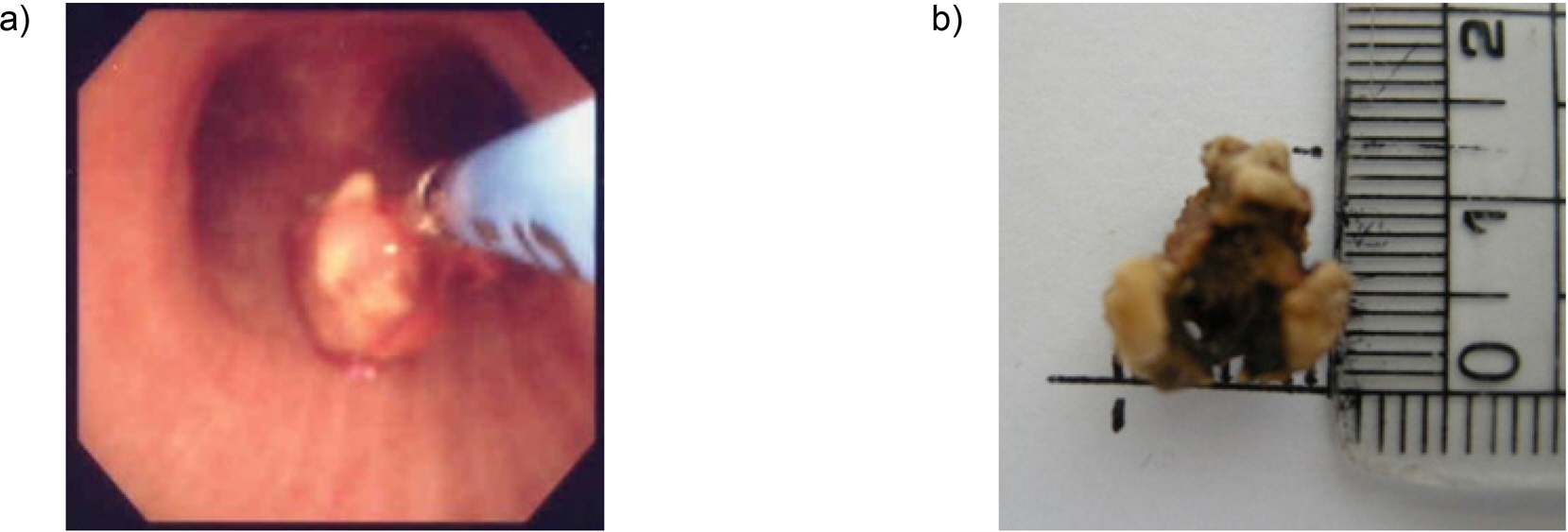
a) Broncholith was removed by cryotherapy through flexible bronchoscopy. b) The length of a removed stone at the right middle bronchus was 1.3 cm. (Reference: A Case of Endobronchial Actinomycosis with Broncholith Removed by Cryotherapy through Flexible Bronchoscopy. Scheduled to be published in Kosin Medical Journal, December of 2013).
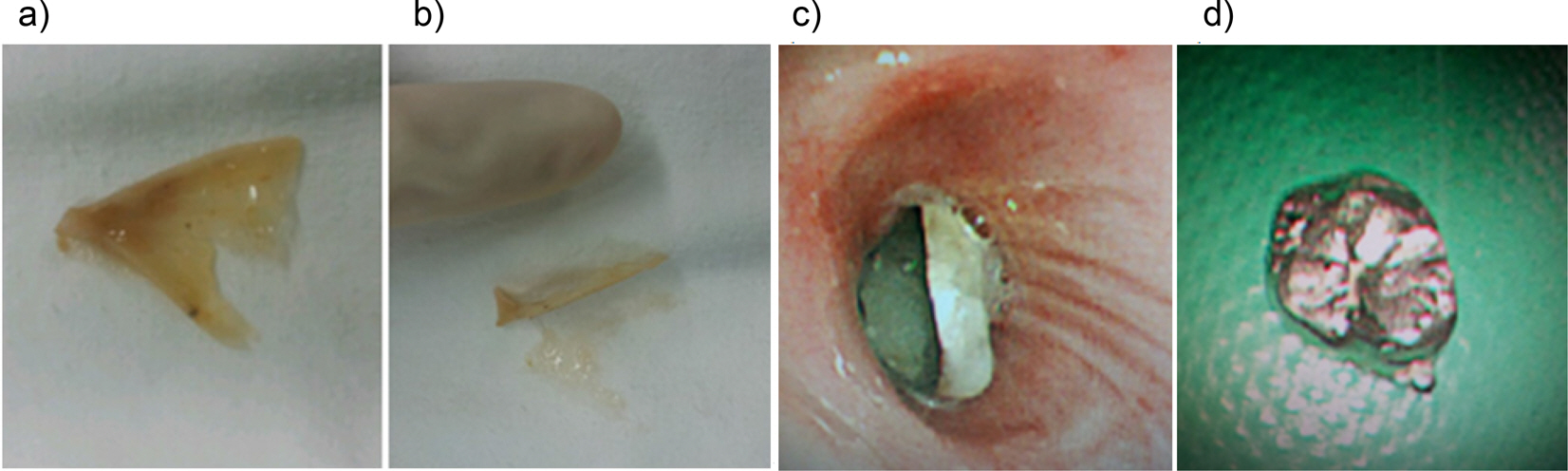
a) A fish bone was extracted from the bronchus. b) Size of the extracted fishbone compared with a human finger tip. c) An impacted artificial tooth crown was seen on bronchoscopy. d) The artificial tooth crown was successfully extracted.
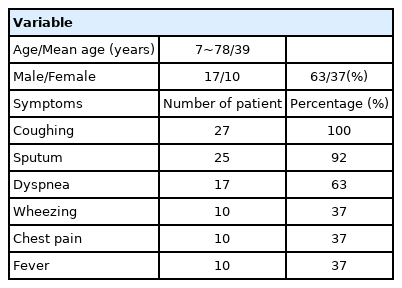
Patient demographics and accompanying symptoms

Location of impacted foreign bodies
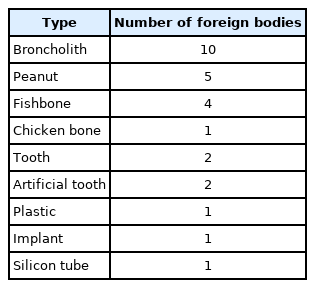
Types of foreign bodies

Removal method and number of foreign bodies