Troponin I and D-dimer levels as triaging biomarkers to distinguish acute pulmonary thromboembolism from myocardial infarction
Article information

Abstract
Background
Acute pulmonary thromboembolism (APTE) is often confused with myocardial infarction. Previous studies have shown that patients with APTE exhibit lower initial and peak cardiac troponin I (CTI) levels, but higher D-dimer (DD) levels, than patients with myocardial infarction. The present study aimed to reaffirm the tree model algorithm using an entirely new set of data.
Methods
We reviewed retrospective clinical and laboratory data from patients who were diagnosed with APTE or non-ST-elevation myocardial infarction (NSTEMI) between 2015 and 2016. Subjects who were not classified with a diagnosis or did not have their CTI or DD levels assessed were excluded. We categorized patients according to the previous algorithm and compared the outcomes with the previous test dataset.
Results
The analysis involved data from 156 patients with APTE and 363 patients with NSTEMI. In the validation data set, the APTE group showed higher initial DD levels (9.80±10.84 μg/mL) and lower initial CTI levels (0.17±0.54 μg/mL) than the NSTEMI group. The accuracy rate for the test dataset and the validation set were similar. The test set accuracy rate was 91.0%, while the accuracy rate in the validation set improved to 88.6%.
Conclusions
Patients with APTE exhibited lower initial and peak CTI levels, but higher DD levels than NSTEMI patients. The accuracy rate estimates were similar between the test set obtained from the tree model algorithm and the validation set. The study findings demonstrate that the assessment of cardiac biomarkers can be useful for differentiating between APTE and NSTEMI.
Introduction
Acute pulmonary thromboembolism (APTE) can lead to death and is often characterized by symptoms such as chest pain, shortness of breath, and elevated levels of cardiac markers such as cardiac troponin I (CTI) and D-dimer (DD) [1-4]. Our prior research demonstrated that subjects with APTE displayed lower initial and peak levels of CTI, while having higher levels of DD compared to patients with non-ST-elevation myocardial infarction (NSTEMI) [5]. Therefore, the assessment of cardiac biomarkers can be useful for differentiating between APTE and NSTEMI, and the tree model algorithm was previously introduced for this purpose [5]. Pulmonary thromboembolism, such as chest pain, dyspnea, and syncope, shares similarities with coronary artery disease, such as myocardial infarction [3,6]. Therefore, when dealing with a patient for the first time, it can be difficult to determine whether to perform a coronary angiogram or a chest computerized computed tomography. We have therefore sought to develop algorithms based on objective markers like CTI and DD.
In this study, our aim was to validate the tree model algorithm in another dataset and investigate a more convenient method of triaging using DD and CTI levels for a differential diagnosis between myocardial infarction and APTE [7].
Methods
Ethical statements: The Institutional Review Board of Dong-A University Hospital granted approval for this protocol (IRB No. DAUHIRB-15-228). The study followed the principles outlined in the Declaration of Helsinki, and the need for informed consent was waived due to the retrospective nature of the chart review design.
1. Data collection and study design
Between January 2015 and December 2016, we gathered historical clinical and laboratory information from individuals who had been diagnosed with APTE and NSTEMI. The presence of APTE was verified through methods such as radionuclide ventilation-perfusion scan, angiography, and chest computed tomography. On the other hand, the diagnosis of NSTEMI was established based on coronary angiography with cardiac biomarkers. Subjects who could not be classified or did not have their CTI and DD levels assessed were excluded. We grouped participants into five different categories based on the tree model algorithm and compared performance to the previous results. The five categories followed the tree algorithm node, and the subjects of the previous study were defined as the test set, and compared with the new validation set recruited in this study.
2. DD assay
The immunoturbidimetric assay enriched with latex is an affordable and swift test, exhibiting analytical sensitivity similar to the traditional enzyme-linked immunosorbent assay (ELISA). To measure DD levels in this study, blood sample taken from a vein was introduced into a test tube containing sodium citrate. Subsequently, the Inovance (Siemens AG) DD assay kit with a Sysmex CS 5100 analyzer (Siemens Medical Solutions) was employed to carry out an immunoturbidimetric assay. A DD concentration of >0.55 mg/L was considered a positive result. For those who had undergone multiple DD evaluations, the initial value obtained before imaging and after the event was used for this analysis.
3. CTI assay
Myocardial ischemia is prevalent among patients with NSTEMI and is indicated by elevated CTI levels. CTI levels were quantified by obtaining venous blood samples in tubes containing heparin and analyzing them twice using the i-STAT system (Abbott Diagnostics). The i-STAT CTI test cartridge used the ELISA method. A CTI concentration of >0.01 μg/mL was considered positive.
4. Description of the tree model algorithm
The tree analysis in this study is a decision tree analysis. It is also known as a tree model. This method is an analysis method that classifies the entire data into several subgroups or performs prediction by representing decision-making rules in a tree structure. It is important to select classification variables and classification reference values at each step of forming a tree structure from an upper node to a lower node. Based on this criterion in the parent node, subnodes diverging from each other are selected so that homogeneity within nodes and heterogeneity between nodes are greatest. Advantages of the tree model include simple structure, easy interpretation, analysis of useful input variables, interaction between predictors and non-linearity, and non-parametric model. In this study, the tree analysis was conducted in R statistical software version 3.4.0.
The algorithm used to discriminate between APTE and myocardial infarction has been described previously [5]. In brief, the algorithm incorporates both baseline high-sensitivity CTI levels and DD levels at the hospital visit. Group 2 is defined as having a baseline CTI level of less than 0.11 μg/mL and a baseline DD level of over 1.5 μg/mL, while group 4 is defined as having a baseline CTI level of less than 0.14 μg/mL and a baseline DD level of over 3.18 μg/mL. The two groups are assumed to reflect APTE. The other groups are more likely to associate with NSTEMI (Table 1, Fig. 1).

Diagnostic performance of the algorithm
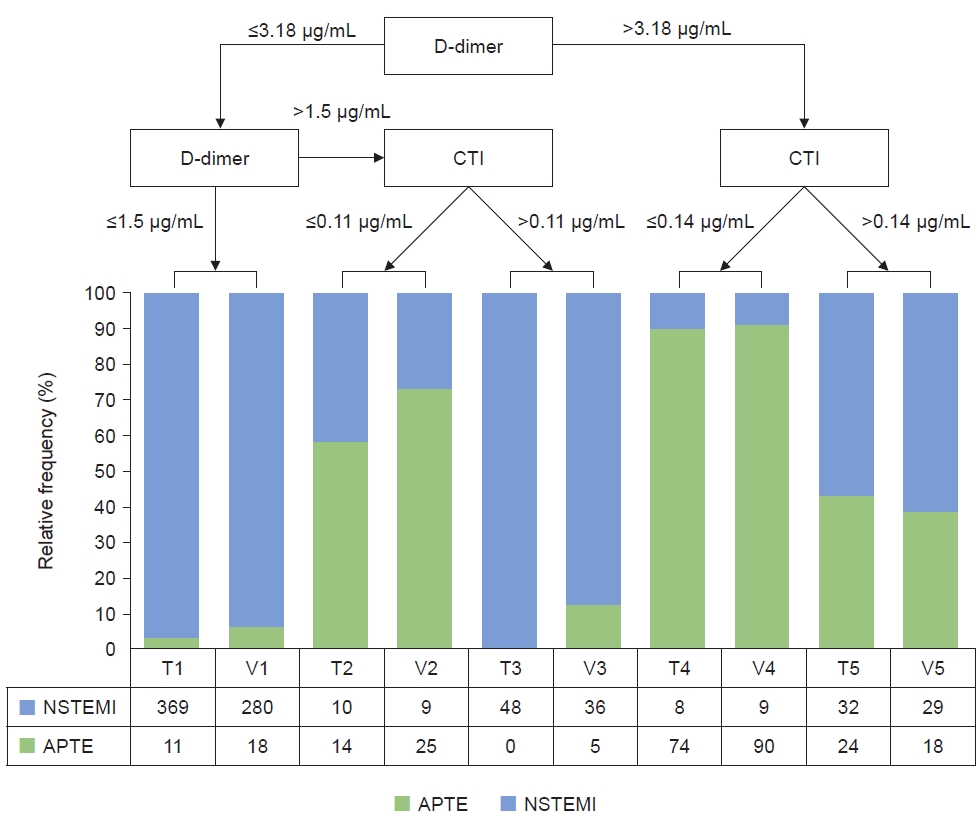
Validation and diagnostic performance of the previous algorithm. The tree model created five groups. When the validation set was matched to the corresponding group and compared with the previous test set, similarities were noted. NSTEMI, non-ST-elevation myocardial infarction; APTE, acute pulmonary thromboembolism; CTI, cardiac troponin I; T, test set; V, validation set.
5. Statistical analysis
Data analysis was performed using SPSS 18.0 (SPSS Inc.). Data were summarized as mean±standard deviation for continuous variables and percentages for categorical variables. The validation population was divided into APTE and NSTEMI groups according to the previous triaging algorithm using initial DD and CTI levels, with a comparison to confirm diagnosis. The diagnostic performance of the algorithm was tested for sensitivity, specificity, predictive values and the area under the receiver operating characteristic curve. A further triaging system was developed on the basis of the previous algorithm and the results of validation. A p-value less than 0.05 was considered to be statistically significant.
Results
1. Study population characteristics
Of the 519 patients who were enrolled in this study, 156 APTE patients were diagnosed using chest computed tomography, and 363 NSTEMI patients were diagnosed using CTI, electrocardiogram, and coronary angiography. All subjects had been assessed for baseline DD and CTI levels. In the APTE group, the mean age was 67.7 years old and 48.1% were male. Thirty-two point seven percent of APTE patients had a malignancy and 30.8% of the APTE patients showed concomitant deep vein thrombosis (DVT). The incidence of diabetes, chronic lung disease, and chronic kidney disease was not significantly different between the two groups. The APTE group showed higher initial DD levels (9.80±10.84 μg/mL) and lower initial CTI levels (0.17±0.54 μg/mL) than the NSTEMI group (Fig. 2), similar to previous results. One case of concomitant myocardial infarction and APTE was excluded from the study. The patient baseline characteristics are presented in Table 2.
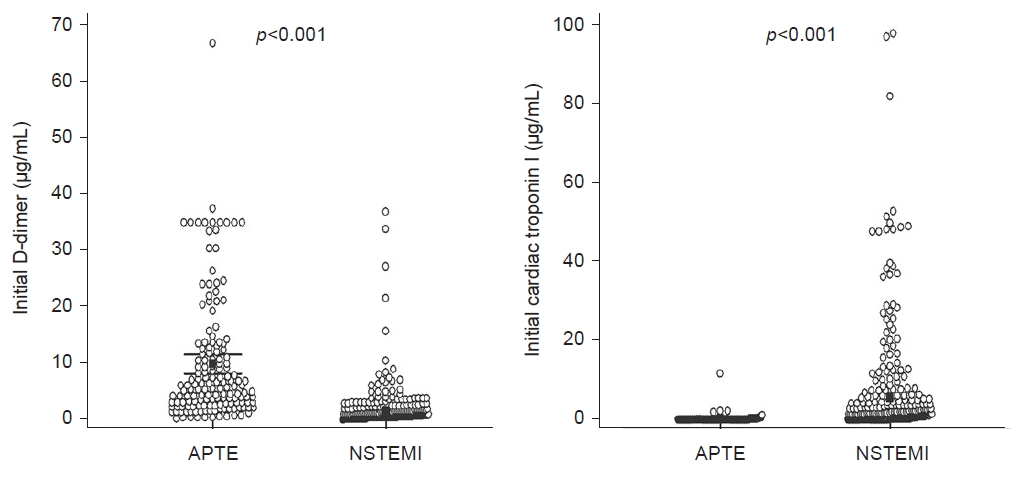
Initial troponin I and D-dimer level in validation data. APTE, acute pulmonary thromboembolism; NSTEMI, non-ST-elevation myocardial infarction.
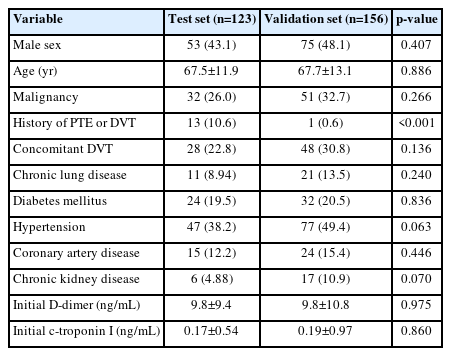
Study population characteristics
2. Diagnostic performance of the algorithm
The diagnostic power was verified in an algorithm mentioned previously [5]. Groups 2 and 4 were assumed to be acute pulmonary embolism, while groups 1, 3, and 5 were regarded as myocardial infarction. The accuracy rate was similar between the test data set and the validation set. The test set accuracy rate was 91.0%, and in the validation set, the accuracy saw an enhancement, reaching 88.6%.
3. Easy guidance for further evaluation in patients with chest pain or dyspnea
Based on previous studies and validation data, we have developed several algorithms that can more easily access the first imaging tools with CTI and DD levels in patients with chest pain and dyspnea. Patients suffering from chest pain or dyspnea are more likely to be diagnosed with myocardial infarction if a DD value of less than 1.5 μg/mL is indicated in the emergency room or a first CTI value of greater than 0.1 μg/mL is indicated, so prompt coronary angiography may be recommended. If the first DD value exceeds 1.5 μg/mL and the CTI value is less than 0.1 μg/mL, the patients may be recommended for chest computed tomography, firstly, for the diagnosis of pulmonary thromboembolism (Fig. 3). It is necessary to further investigate the utility of this technique in the future. However, the aim of this study was to help differentiate between myocardial infarction and pulmonary embolism.
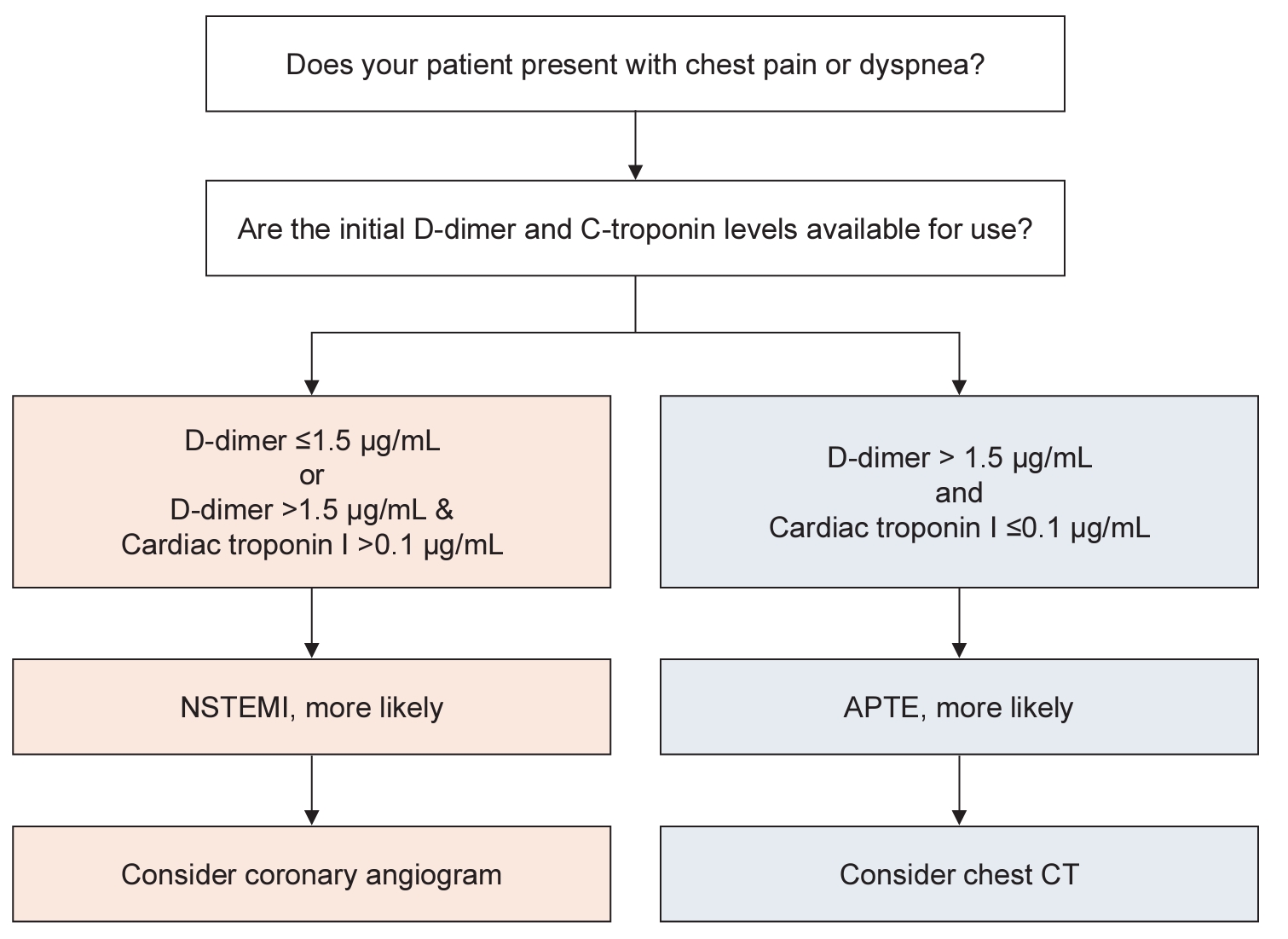
Decision-making tree for rapid diagnosis of APTE or NSTEMI. APTE, acute pulmonary thromboembolism; NSTEMI, non-ST-elevation myocardial infarction; CT, computed tomography.
Discussion
This study verified differences in initial CTI and DD levels present in patients presenting with myocardial infarction versus APTE, and appears useful for initial discrimination. Our previous study described the discriminating algorithm used [5]. We have now further proposed guidance for the initial diagnostic strategy in practice where NSTEMI or APTE are suspected, with both conditions requiring rapid diagnosis and management [8,9]. Although clinical characteristics are important in diagnosis, it can be difficult to make decisions dependent on prior diagnostic tests, and whether coronary angiography or computed tomography is needed. We believe the findings in the present study may be helpful for differential diagnosis and initial evaluation using a more simplified classification.
Several previous studies have demonstrated that DD levels increase during myocardial infarction [10], and it has been widely reported that CTI increases during pulmonary embolism and is associated with prognostic outlook [2]. The mechanisms responsible for myocardial infarction and pulmonary embolism are distinct because the mechanisms behind arterial thrombosis and venous thrombosis are also different. CTI and DD levels can be indicative of such differences. The current recommended therapy for pulmonary thromboembolism is thrombolysis and anticoagulation, but because bleeding complication risk is high (similar to the treatment of myocardial infarction), rapid diagnosis is crucial. The clinical features and clinical significance of DD levels in pulmonary embolism reveal that in the group with elevated levels, the actual diagnosis of pulmonary thromboembolism was only 30.6% in the DD-positive group (674 of 2,199 subjects). Conversely, others in the DD-positive group were ruled out as having APTE upon further evaluation or remained as an inconclusive diagnosis. In addition, five of 1,057 subjects with DD negative status experienced venous embolic events during the 3-month follow-up [11]. Therefore, careful differential diagnosis is important, and it is difficult to exclude APTE mimicking myocardial infarction. Despite efforts to increase the sensitivity and specificity of these diagnoses, in the tree model group 5, when DD >3.18 μg/mL and CTI >0.14 μg/mL, APTE was about 60%, and cases were not well differentiated. This suggests that additional research is needed.
Although the usefulness of the coagulation test (including DD levels) in the diagnosis of myocardial infarction remains controversial, it has been confirmed that it can aid in the differential diagnosis of pulmonary embolism and myocardial infarction [12-19]. In contrast, in critical care units, DD levels are frequently elevated due to heart failure or other diseases, and for this reason it has been reported to be less informative than fast echocardiography [4]. Although early echocardiographic evaluation is also important, there is a limitation associated with emergency screening as delays are common due to a frequent lack of skilled ultrasonographers.
A previous study showed that the ratio of DD to CTI showed better sensitivity and specificity in the differential diagnosis between APTE and NSTEMI than either DD or CTI [20]. The peculiarity of this study emphasized that DD is a test with high specificity in diagnosing APTE in general. The study more focused on sensitivity, but in this study, it would be meaningful to further increase the existing DD specificity through DD and CTI combination.
This study focused on uniform biomarkers, and the clinical data collection was all performed within one university center. All subjects had their diagnoses confirmed by imaging studies. The majority of subjects were verified as having pulmonary thromboembolism by multi-detector computed tomography. Only one case of pulmonary embolism in the test set received a lung perfusion scan for diagnosis. Therefore, the likelihood of over diagnosis or a low detection rate appears low. Previous study reported 40.0% to 50.0% of patients with DVT have APTE, and 90.0% of patients with APTE are diagnosed with DVT. However, in this study, the rate was lower at 30.8%. This study is a retrospective study, and has a limitation of not collecting information on DVT tests in all patients [21]. As this study was performed retrospectively, the patients were not randomized. Some of the NSTEMI and APTE cases showed elevated CTI and D-D levels, and further investigation of these findings is needed.
In conclusion, our findings suggest that the assessment of cardiac biomarkers can be useful when differentiating APTE from NSTEMI. Patients with APTE exhibit lower initial and peak CTI levels, but higher DD levels than NSTEMI patients. In this study, the estimated accuracy rates were similar between the test set derived from the tree model algorithm and the validation set. Patients with DD levels below 1.5 μg/mL or over 0.1 μg/mL of CTI were relatively unlikely to be harboring APTE (specificity 95.3%). These results demonstrate that assessing initial CTI and DD levels can be useful for ruling out APTE in emergency scenarios.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Author contributions
Conceptualization: MHK. Data curation: SJK, JWL, YSC, DEK, JYH. Formal analysis: KML. Investigation: SJK. Methodology: SJK, KML. Project administration: MHK. Resources: SJK. Software: SKK, KML. Supervision: MHK, JSP. Validation: SJK, KML. Visualization: SJK, KML. Writing – original draft: SJK. Writing – review & editing: SJK, MHK.