 KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Volume 33(1); 2018 > Article
-
Original Article
Effect of Computerized Neuropsychologic Test in Subacute Post-Stroke Patient With Cognitive Impairment - Chang Hwa Lee, Won Sik Moon, Yong Hyun Han, Po Sung Jun, Gi Hun Hwang, Ho Joong Jung
-
Kosin Medical Journal 2018;33(1):51-63.
DOI: https://doi.org/10.7180/kmj.2018.33.1.51
Published online: June 30, 2018
1Department of Rehabilitation Medicine, Dong-eui Medical Center, Busan, Korea.
2Department of Physical Medicine and Rehabilitation, College of Medicine, Kosin University, Busan, Korea.
- Corresponding Author: Ho Joong Jung, Department of Physical Medicine and Rehabilitation, College of Medicine, Kosin University, 262, Gamcheon-ro, Seo-gu, Busan 49267, Korea. Tel: +82-51-990-6481, Fax: +82-51-990-2019, jhjpmr@naver.com
• Received: August 30, 2016 • Revised: November 16, 2016 • Accepted: December 21, 2016
Copyright © 2018 Kosin University College of Medicine
- 1,309 Views
- 4 Download
Abstract
-
Objectives
- To investigate the effects of Computerized Neuropsychologic Test (CNT) on cognitive function and daily life performance in subacute post-stroke patients with cognitive impairment.
-
Methods
- Korean Mini-Mentals State Examination (K-MMSE), Korean version of Modified Barthel Index (K-MBI) were investigated in 125 subacute post-stroke patients with cognitive impairment. We analyzed K-MMSE and K-MBI which were conducted 63 patients who had received CNT and 62 patient who had not received CNT from baseline to 8 weeks follow-up. In the experimental group, initial K-MMSE and K-MBI were conducted 13.3 ± 6.8 weeks after the onset of stroke and their age was 63.4 ± 13.3. In the control group, initial K-MMSE and K-MBI were conducted 13.2 ± 7.7 weeks after the onset of stroke and their age was 65.1 ± 11.6.
-
Results
- The 8 weeks follow-up total K-MMSE score and total K-MBI score of experimental group were significantly higher than control group (P < 0.05). In K-MMSE subsection, orientation, judgement, recall, language & visual reconstruction were significantly higher in experimental group than control group (P < 0.05). In K-MBI subsection, personal hygiene, bathing self, toilet, dressing, ambulation, chair/bed transfer were significantly higher in experimental group than control group (P < 0.05). The change of total K-MMSE score of experimental group was significantly correlated with change of total K-MBI score (P < 0.05), but control group was not (P > 0.05). In K-MMSE subsection, change of orientation, registration, language and visual reconstruction were correlated with total K-MBI s core after CNT. Especially, the experimental group, total K-MBI score of the left hemisphere damage group was significantly higher than the right hemisphere damage group (P < 0.05).
-
Conclusions
- This study shows that CNT is effective on subacute post-stroke patients with cognitive impairment. Improvement of cognitive function can expect a positive outcome on daily life performance, in particular, it can be expected to improve the prognosis of patients with stroke, the left hemisphere lesions.
- Subjects
- The subject for this study were 125 patients who scored less than 23 points in K-MMSE among the subacute stroke patients who received treatment at 00 Hospital as inpatients or outpatients for less than 6 months after a stroke. 63 patients who underwent CNT were included in the experimental group and 62 patients who did not were included in the control group. The cerebral infarction and cerebral hemorrhage were confirmed based on the results of brain magnetic resonance imaging (MRI) and brain computed tomography (CT) scanning. Both the experimental group and control group were taking Donepezil (5 mg/day for 28 days, followed by 10 mg/day). The patient with speech impediment and aphasia, the patients with hearing disorder, the patients with neuropsychiatric disorders and the patients who suffered the diseases (e.g. dem entia, drug addition, etc.) that might cause cognitive dysfunction before the onset of stroke were excluded from the subjects for this study. In the experimental group, there were 37 cerebral infraction patients and 26 cerebral hemorrhage patients in the experimental group. For the lesion site of stroke, 25 patients had a stroke in the right cerebral hemisphere and 38 patients had a stroke in the left cerebra hemisphere. Initial K-MMSE and K-MBI were conducted 13.3 ± 6.8 weeks after the onset of stroke and their age was 63.4 ± 13.3. In the control group, there were 39 cerebral infraction patients and 23 cerebral hemorrhage patients in the experimental group. For the lesion site of stroke, 25 patients had a stroke in the right cerebral hemisphere and 37 patients had a stroke in the left cerebral hemisphere. Initial K-MMSE and K-MBI were conducted 13.2 ± 7.7 weeks after the onset of stroke and their age was 65.1 ± 11.6. There was no statistically meaningful difference in the legion site of stroke and the period to the initial test (Table 1). The study was conducted after obtaining an approval of IRB of 00 Hospital.
- Methods
- This study is a retrospective case - control study. The medical records of all the subjects were examined and then the general characteristics of them and K-MMSE and K-MBI data were analyzed. To evaluate the cognitive functions of the subjects before the implementation of CNT, K-MMSE performed at the start of CNT was examined, and then K-MMSE performed 8 weeks after the implementation of CNT was examined to evaluate the cognitive functions of the subjects after the implementation of CNT, K-MMSE performed 8 weeks after the implementation of CNT was examined. In this study, K-MMSE total score (on a scale of 30) and 6 sub items (i.e. orientation, registration, calculation, judgment, recall, language and visual reconstruction) were examined.
- Additionally, the K-MBI performed at the start of CNT and the K-MBI performed 8 weeks after the implementation of CNT for the two groups were examined. In this study, K-MBI total score (on a scale of 100) and 10 sub items (i.e. personal hygiene, bathing self, feeding, toilet, stair climbing, dressing, bowel control, bladder control, ambulation, wheelchair, chair/bed transfer) were examined.
- For the experimental group, CNT was performed using Seoul Computerized Neuropsychological Test. For the CNT sub-items, a total of 10 items (i.e. Digit span forward test for verbal memory evaluation; Digit span backward test; Verbal learning test; Visual span forward test for visuospatial memory evaluation; Visual span backward test, Visual learning test; Auditory Continuous performance test (CPT) for attention evaluation; Visual CPT test and Trail making test set A, B for visual motor integration ability) were performed (Table 2). Computerized neuropsychological tests were performed for 8 weeks, 2 sessions per week and for 30 minutes per session. Additionally, for the two groups, conventional rehabilitation treatment including physical therapy and occupational therapy (twice a day, 5 times per a week, for 8 weeks), and Donepezil treatment were performed.
- A statistical analysis was performed using the SPSS 18.0 for windows MS. Additionally, the both groups were compared between before and after the treatment using a paired t-test, and the differences between the two groups were compared using a student t-test. To compare the correlation between the variation in K-MMSE sub-items and the variation in K-MBI total score for both groups, Pearson correlation was used, with the significance level set at < 0.05.
MATERIALS AND METHODS
- K-MMSE and K-MBI for the experimental group and control group before the implementation of CNT
- K-MMSE total average score before the implementation of CNT was 17.29 ± 5.82 points in the experimental group and 17.81 ± 8.07 points in the control point, indicating there is no statistically meaning differences between the two groups. Additionally, in all 6 items of K-MMSE sub-items (i.e. orientation, registration, calculation, judgment, recall, language and visual reconstruction), no item showed statistically meaningful difference between the two groups. K-MBI total average score before the implementation of CNT was 37.14 ± 24.91 points and 38.08 ± 20.04 points in the experimental group and the control group respectively, indicating that there was no statistically meaningful difference between the two groups. In 8 items of K-MBI sub-items (i.e. personal hygiene, bathing self, feeding, toilet, stair climbing, dressing, ambulation, wheelchair, chair/bed transfer), there was no statistically meaningful difference between the two groups, whereas in two items: bowel control and bladder control, statistically meaningful difference was observed.
- K-MMSE and K-MBI for the experimental group and control group after the implementation of CNT
- K-MMSE total score of the experimental group after the implementation of CNT was 23.03 ± 4.85 points, indicating an increase of 5.74 ± 3.66 points compared to before treatment and K-MMSE total score of the control group was 20.57 ± 9.68 points 8 weeks after the initial evaluation, indicating an increase of 2.76 ± 5.37 points compared to the initial evaluation, so both groups showed meaningful improvement. In 6 K-MMSE sub-items (i.e. orientation, registration, calculation, judgment, recall, language and visual reconstruction), statistically meaningful improvement was observed.
- K-MBI total score in the experimental group was 58.83 ± 21.83 points, an increase of 21.68 ± 12.50 points compared to before the treatment, and K-MBI total score in the control group was 51.05 ± 22.13 points, an increase of 13.03 ± 15.55 points compared to the initial evaluation, so both groups showed statistically meaningful improvement. In 10 items of K-MBI sub-items items (i.e. personal hygiene, bathing self, feeding, toilet, stair climbing, dressing, bowel control, bladder control, ambulation, wheelchair, chair/bed transfer), both groups showed meaningful improvement (Table 3). The results of a comparative analysis of K-MMSE total scores and the scores in the sub-items between the two groups demonstrated that the experimental group showed a statistically meaningful improvement in K-MMSE total score and 4 sub-items (i.e. orientation, judgment, recall, language and visual reconstruction) compared to the control group, whereas in 2 items (i.e. registration, calculation), no statistically meaningful difference between the two groups was observed (Table 4). The results of a comparative analysis of the two groups after the implementation of CNT demonstrated that 6 sub-items (i.e. personal hygiene, bathing self, toilet, dressing, ambulation, chair/bed transfer) showed statistically meaningful improvement, whereas 4 sub-items (i.e. feeding, stair climbing, bowel control and bladder control) showed no statistically meaningful difference between the two groups (Table 5).
- The results of a comparative analysis of the two groups according to the cause of stoke showed that both the cerebral hemorrhage group and the cerebral infraction group in the experimental group showed an improvement in K-MMSE and K-MBI total score compared to those in the control group whereas the results of an analysis in the experimental group showed no meaningful difference between the cerebral hemorrhage group and the cerebral infraction group of both groups. The results of an analysis of lesion site of stroke in the experimental group demonstrated that the left cerebral hemisphere damaged group in the experimental group showed a meaningful improvement in K-MBI total score compared with the right cerebral hemisphere damaged group whereas the control group showed no meaningful difference. For K-MMSE total score, there was no meaning difference between the right cerebral hemisphere damaged group and the left cerebral hemisphere damaged group of both groups (Table 6).
- Correlation between the variation of K-MMSE and K-MBI before and after the implementation of CNT
- The correlation between the variation of K-MMSE and K-MBI before and after the implementation of CNT was examined. In the experimental group, statistically meaningful positive correlation between the variation of K-MMSE and K-MBI before and after the implementation of CNT was observed, whereas in the control group, no statistically meaningful correlation was observed (Table 7). In the experimental group in which statistically meaningful correlation was observed, the correlation between the variation of K-MMSE sub-items and the variation of K-MBI total score was analyzed. The results demonstrated that there was meaningful correlation between the variation of 3 items (i.e. orientation, registration and language and visual reconstruction) and the variation of K-MBI total score (Table 8).
RESULTS
- Stroke is a major cause of mortality and disability worldwide, it was reported that the frequency of cognitive and perceptual impairments in the patients who experienced a stroke more than 3 months ago vary from 13.6 to 39%, and up to a third of them develop dementia.14 In the cognitive rehabilitation, it is critical to evaluate the patients with cognitive dysfunction in the early stage and establish treatment plans by determining the impaired cognitive domains.15 Although the effect of CNT is generally agreed, yet the evidences for treatment are still disputable. Currently many studies reported the positive effect of CNT on the cognitive rehabilitation for brain damaged patients and the clinical usefulness of CNT is gradually increasing. It has been known that the improvement of cognitive function in the stroke patients has a positive effect on the functional recovery.16 Additionally, it has been reported that the implementation of CNT leads to the improvement of cognitive function.13 Therefore, if the improvement of cognitive function can be expected through the implementation of CNT, better functional recovery can be also expected.
- The results of this study demonstrated that only physical therapy, occupational therapy and drug therapy for the subacute stroke patients with accompanying cognitive impairment resulted in an improvement in K-MMSE and K-MBI, and if the therapy is coupled with CNT, better functional recovery could be expected. Additionally, when CNT was implemented, with an increase in K-MMSE score, M-MBI score tended to increase.
- According to Kim et al.,13 conventional rehabilitation coupled with CNT was conducted for 4–6 weeks for the chronic patients who suffered brain damage for more than 12 months and the results showed an improvement in short-term verbal memory, short-term visual perception memory, auditory and visual attention concentration. Hogarty and Flesher et al. reported in their study that the mental patients with accompanying cognitive impairment showed a meaningful improvement in attention17 problem solving ability and social cognition and disability evaluation after the implementation of “Cognitive Enhancement Therapy” using CNT for 1 year. Bell et al. also reported that the partly computerized CNT resulted in improvements in working memory and executive function compared to conventional occupational therapy.18 In this study, in K-MMSE total score, the experimental group showed statistically meaningful improvements compared to the control group, and between the sub-items, a statistically meaningful improvement was observed in orientation, judgment, recall, language and visual reconstruction. It seems that repetitive learning of language memory, spatiotemporal memory, attention function evaluation, Visuo-motor coordination, and Visuo-motor cognitive capacity test helps to increase the score of these areas. When compared with the study by Hogarty and Flesher et al., there are similarities in the overall cognitive function improvements, yet there are differences in the improved sub-items. In addition, in this study, the results of a comparative analysis of two groups and the K-MMSE sub-items improved in the experimental group were consistent with those in the study by Bell et al.
- In this study, it was observed that the sub-acute stroke patients with accompanying cognitive impairment showed higher improvements in K-MBI total score after the implementation of CNT compared to the control group. Among the sub-items, higher improvements were observed in 6 sub-items (i.e. personal hygiene, bathing self, toilet, dressing, ambulation, chair/bed transfer). The improvement of the score in the executive function area including the ambulation in K-MBI is considered to be an increase of the overall score of MMSE, and it is thought to be related to CNT that include spatiotemporal memory, attention function evaluation, Visuo-motor coordination, and Visuo-motor cognitive capacity test. Han et al reported in their study that the results of the examination of the cognitive condition of the patients with cognitive impairment using walking and MMSE showed that the MMSE total score indicating the overall degree of cognitive area rather than the importance of individual cognitive domains is more clearly associated with walking, and walking ability may relate to the higher level cognitive functions including executive function.19 Kim et al said in their study that Functional Ambulatory Category (FAC) indicating the independent walking level of the stroke patients when leaving the hospital after receiving rehabilitation treatment showed the meaningful amount of correlation with MMSE and MBI, supporting the argument that higher level cognitive functions relate to walking ability.20 In this study, the improvements in the cognitive functions after the implementation of CNT led to the improvements in the independent life and walking ability of the patients, yet no improvement was observed in climbing stairs. This indicates that the improvements in cognitive functions have a positive effect on walking on even ground level, yet it is not enough for higher level walking (e.g. stair climbing, etc.). In the studies conducted in the past, it was said that the brain language center is located in the left cerebral hemisphere known to be the dominant hemisphere and verbal short-term memory is main undertaken by the left pre-frontal lobe.2122 In this study, the left cerebral hemisphere damaged patients group showed a meaningful improvement in K-MBI total score after the implementation of CNT compared to the right cerebral hemisphere damaged patients group. This result supports that CNT is more effective for the left cerebral hemisphere damaged patients with accompanying impairments in memory and verbal ability among cognitive abilities. However, the difference in K-MBI and K-MMSE between the cerebral hemorrhage group and the cerebral infarction group for both the experimental group and the control group, indicating that the lesion site rather than the causes of a stroke is more critical in predicting the cognitive functions and the ability to perform daily activities. For the limitations of this study, a retrospective research method of reviewing medical records was used, which may lead to a bias, and this study was a single-center study. Therefore, in order to obtain more accurate conclusions, there is the necessity of a large-scale prospective research which will enable it to obtain a large amount of information based on the information from the hospitals in many different areas. Additionally, the control group did not receive the additional treatment for the period of cognitive treatment for the experimental group. If computer related works, which do not relate to other cognitive functions, are performed for the period which is the same as the period of CNT treatment, it is expected to produce better results. For another limitation, K-MMSE and K-MBI have the limitations in the evaluation of the performance of daily activities and only a single evaluation tool was used. K-MMSE is able to evaluate the cognitive functions comprehensively, but it is hard to control conditions during test process, which may result in errors in scoring and recording, or K-MMSE may cause the testers who lack experiences to make less objective decisions. K-MBI also has the limitation in that it evaluates only the ability to perform daily activities through an interview with the patients or the guardians so does not reflect socio-cognitive elements. Therefore, to supplement the limitations in this study, there is the necessity of complementary researches using a wide range of evaluation approaches.
- CNT was performed for the subacute stroke patients with accompanying cognitive impairments. When compared with the control group, the experimental group showed improvements in cognitive functions and the abilities to perform daily activities. These results indicate that the implementation of CNT improves the cognitive functions, which in turn improves the abilities to perform daily activities, particularly for the left cerebral hemisphere damaged patients. Therefore, active CNT treatment for the subacute stroke patients with accompanying cognitive impairments, particularly, for the patients with the lesions in the left cerebral hemisphere, is expected to be able to produce better functional improvements.
DISCUSSION
- 1. Cicerone KD, Dahlberg C, Kalmar K, Langenbahn DM, Malec JF, Berquist TF, et al. Evidence-based cognitive rehabilitation: recommendations for clinical practice. Arch Phys Med Rehabil 2000;81:1596–1615.ArticlePubMed
- 2. Gontkovsky ST, McDonald NB, Clark PG, RuWe WD. Current directions in computer-assisted cognitive rehabilitation. NeuroRehabilitation 2002;17:195–199.ArticlePubMed
- 3. Tatemichi TK, Desmond DW, Mayeux R, Paik M, Stern Y, Sano M, et al. Dementia after stoke: baseline frequency, risks, and clinical features in a hospitalized cohort. Neurology 1992;42:1185–1193.ArticlePubMed
- 4. Rasquin SM, Lodder J, Ponds RW, Winkens I, Jolles J, Verhey FR. Cognitive functioning after stroke: a one-year follow-up study. Dement Geriatr Cogn Disord 2004;18:138–144.ArticlePubMed
- 5. Lezak ML. Neuropsychological assesment. 3rd ed. New York: Oxford University Press; 1995. p. 22–44.
- 6. Diamond PT, Felsenthal G, Macciocchi SN, Butler DH, Lally Cassady D. Effect of cognitive impairment on rehabilitation outcome. Am J Phys Med Rehabil 1996;75:40–43.PubMed
- 7. Folstein MF, Fostein SE, McHugh PR. “Mini-Mental State”. A practical mothod for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189–198.PubMed
- 8. Park JH, Kwon YC. Modification of the mini-mental state examination for use in the elderly in a non-western society Part 1 Development of Korean version of Mini-Mental State Examination. Int J Geriatr Psychiatry 1990;5:381–387.Article
- 9. Kang Y, Na DL, Han S. A validity study on the Korean mini-mental state examination. J Korean Neurol Assoc 1997;15:300–308.
- 10. Kim DH, Na DL, Yeon BG, Kang YW, Min KB, Lee SH, et al. Prevalence of dementia in the elderly of an urban community in Korea. Korean J Prev Med 1999;32:306–316.
- 11. Jung HY, Park BK, Shin HS, Kang YK, Pyun SB, Paik NJ, et al. Development of the korean version of modified barthel index (K-MBI): Multi-center study for subjects with stroke. J Korean Acad Rehabil Med 2007;31:283–297.
- 12. Bellucci DM, Glaberman K, Haslam N. Computer-assisted cognitive rehabilitation reduces negative symptoms in the severely mentally ill. Schizophr Res 2003;59:225–232.ArticlePubMed
- 13. Kim YH, Ko MH, Seo JH, Park SH, Kim KS, Jang EH, et al. Effect of computer-assisted cognitive rehabilitation program for attention training in brain injury. J Korean Acad Rehabil Med 2003;27:830–839.
- 14. Nichols TE, Holmes AP. Nonparametric permutation tests for functional neuroimaging: A primer with examples. Hum Brain Mapp 2002;15:1–25.ArticlePubMed
- 15. Kim JH, Han TR. Rehabilitation medicine. 5th ed. Seoul: Koonja Publishing; 2014. p. 69–70.
- 16. Han TR, Kim JH, Seong DH, Chun MH. The correlation of the Mini-Mental State Examination MMSE and functional outcome in the stroke patients. J Korean Acad Rehabil Med 1992;16:118–122.
- 17. Hogarty GE, Flesher S. Practice principles of cognitive enhancement therapy for schizophrenia. Schizophr Bull 1999;25:693–708.ArticlePubMed
- 18. Bell M, Bryson G, Greig T, Corcoran C, Wexler BE. Neurocognitive enhancement therapy with work therapy: effects on neuropsychological test performance. Arch Gen Psychiatry 2001;58:763–768.ArticlePubMed
- 19. Han JH, Lee SW, Park KW. The association of gait disturbance and cognitive impairment. Dement Neurocognitive Disord 2013;12:94–99.Article
- 20. Kim DY, Park CI, Chang WH, Ahn SY, Ohn SH. Prediction of functional outcome after stroke using acute clinical factors. J Korean Acad Rehabil Med 2003;27:641–646.
- 21. Damasio H, Grabowski TJ, Tranel D, Hichwa RD, Damasio AR. A neural basis for lexical retrieval. Nature 1996;380:499–505.ArticlePubMed
- 22. Démonet JF, Chollet F, Ramsay S, Cardebat D, Nespoulous JL, Wise R, et al. The anatomy of phonological and semantic processing in normal subjects. Brain 1992;115:1753–1768.ArticlePubMed
References
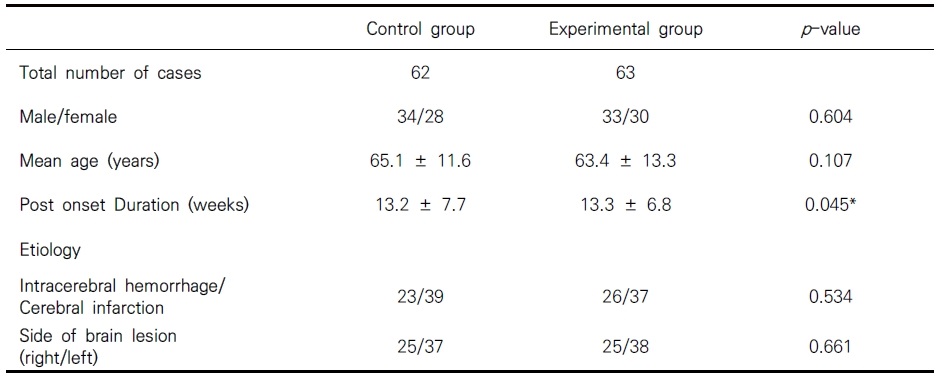
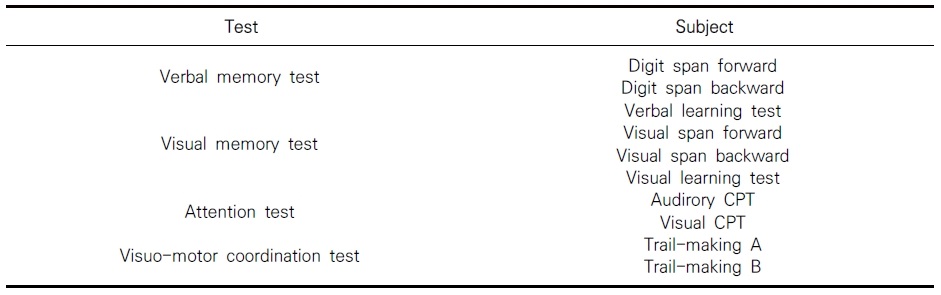
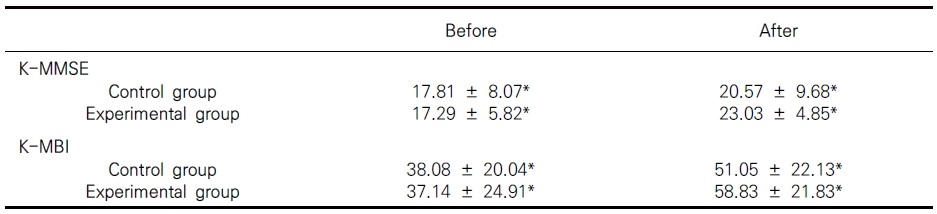
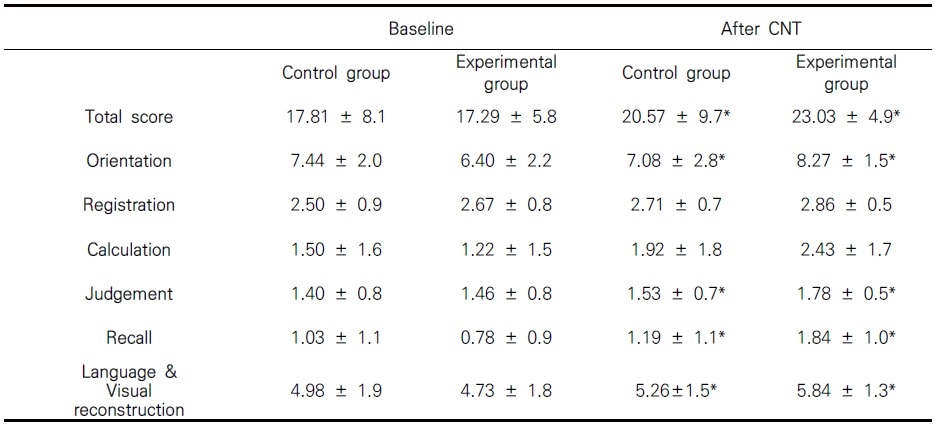
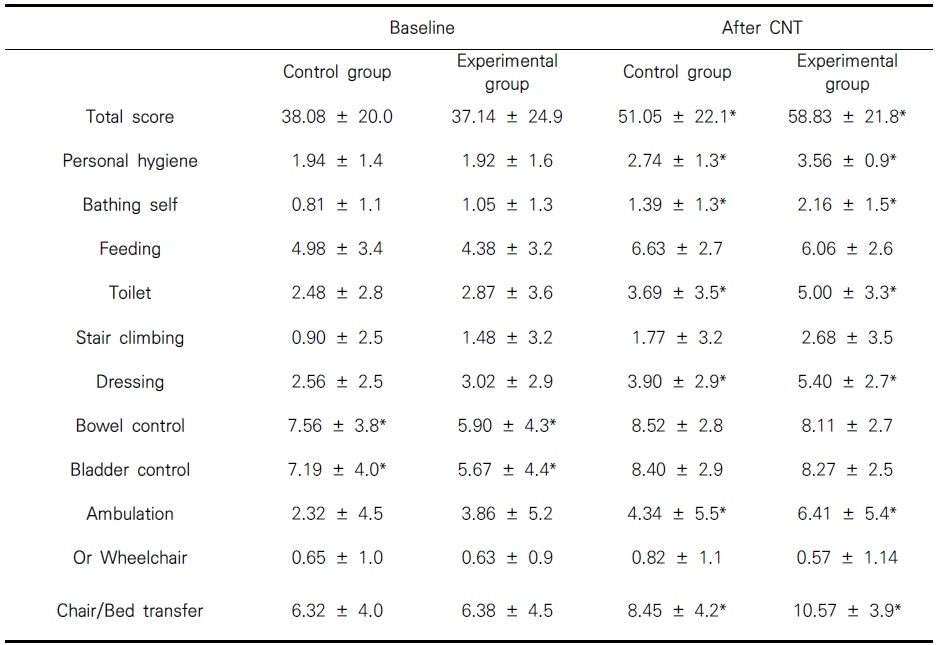
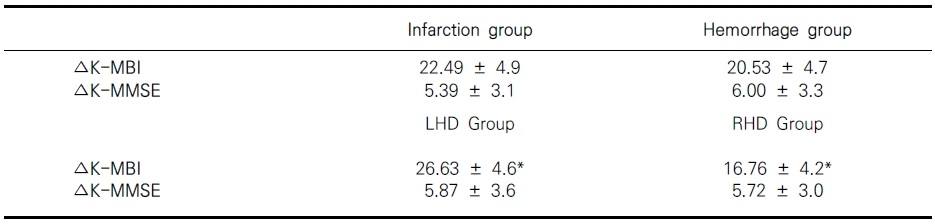
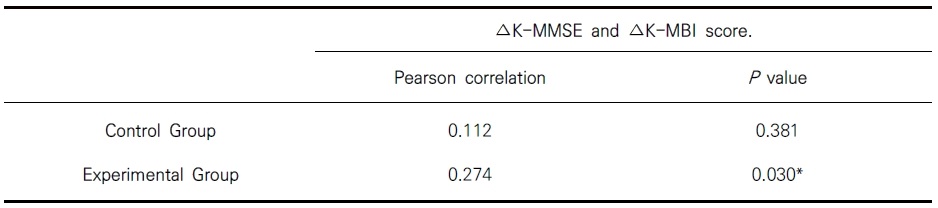
Table 8
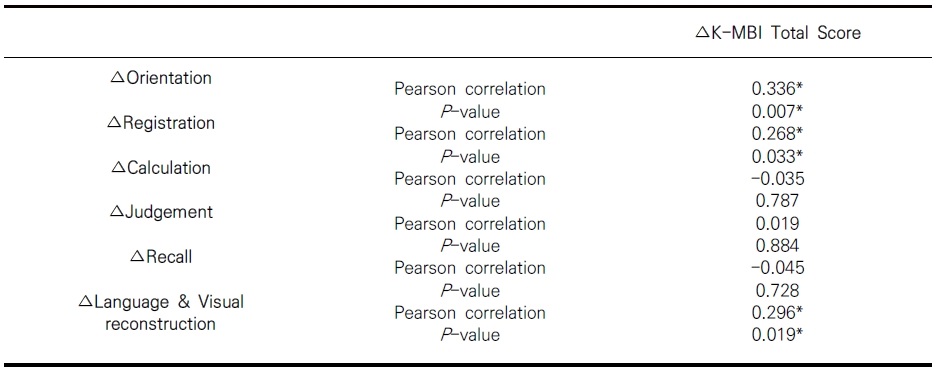
Correlation analysis of ΔK-MMSE subsection and ΔK-MBI total score in experimental group.
*Significance level is p < 0.05; ΔK-MMSE, Change of total K-MMSE score; ΔK-MBI: Change of total K-MBI score; ΔOrientation, Change of orientation score; ΔRegistration, Change of registration score; Calculation, Change of calculation score; ΔJudgement, Change of judgement score; ΔRecall, Change of recall score; ΔLanguage & Visual reconstruction, Change of Language & Visual reconstruction score.
Figure & Data
References
Citations
Citations to this article as recorded by 
 PubReader
PubReader Cite
Cite