KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Volume 30(1); 2015 > Article
-
Original Article
Therapeutic comparison of Surgery combined with chemotherapy and chemotherapy alone for Primary Gastrointestinal Lymphoma: A single center study - Je Hun Kim, Ho Sup Lee, Jun Seop Lee, Jin Young Lee, Su Young Kim, Cheol Su Kim, Joung Wook Yang, Ga In You
-
Kosin Medical Journal 2015;30(1):29-39.
DOI: https://doi.org/10.7180/kmj.2015.30.1.29
Published online: January 20, 2015
Department of Internal Medicine, College of Medicine, Kosin University, Gospel Hospital, Busan, Korea
- Corresponding Author:Ho Sup Lee, Department of Internal Medicine, College of Medicine, Kosin University, Gospel Hospital, 262, Gamcheon-ro, Seo-gu, Busan, Korea TEX: +82-51-990-5820 FAX: +82-51-990-5821 E-mail: hs3667@hanmail.net
• Received: October 13, 2013 • Accepted: June 3, 2014
Copyright © 2015 Kosin University School of Medicine Proceedings
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 942 Views
- 2 Download
Abstract
-
Objectives
- There is still no consensus on the optimal treatment for primary gastrointestinal lymphoma (PGIL). The aim of this study was to compare surgery combined with chemotherapy and chemotherapy alone in PGIL.
-
Methods
- We retrospectively reviewed and analyzed the treatment outcomes of 107 patients with primary gastrointestinal lymphoma diagnosed between March 1999 and December 2009 at Kosin University Gospel Hospital. Patients were divided into two groups: 35 patients who underwent surgery combined with chemotherapy (group A) and 72 patients who were treated with chemotherapy alone (group B). And we analyzed prognostic factors associated with short survival.
-
Results
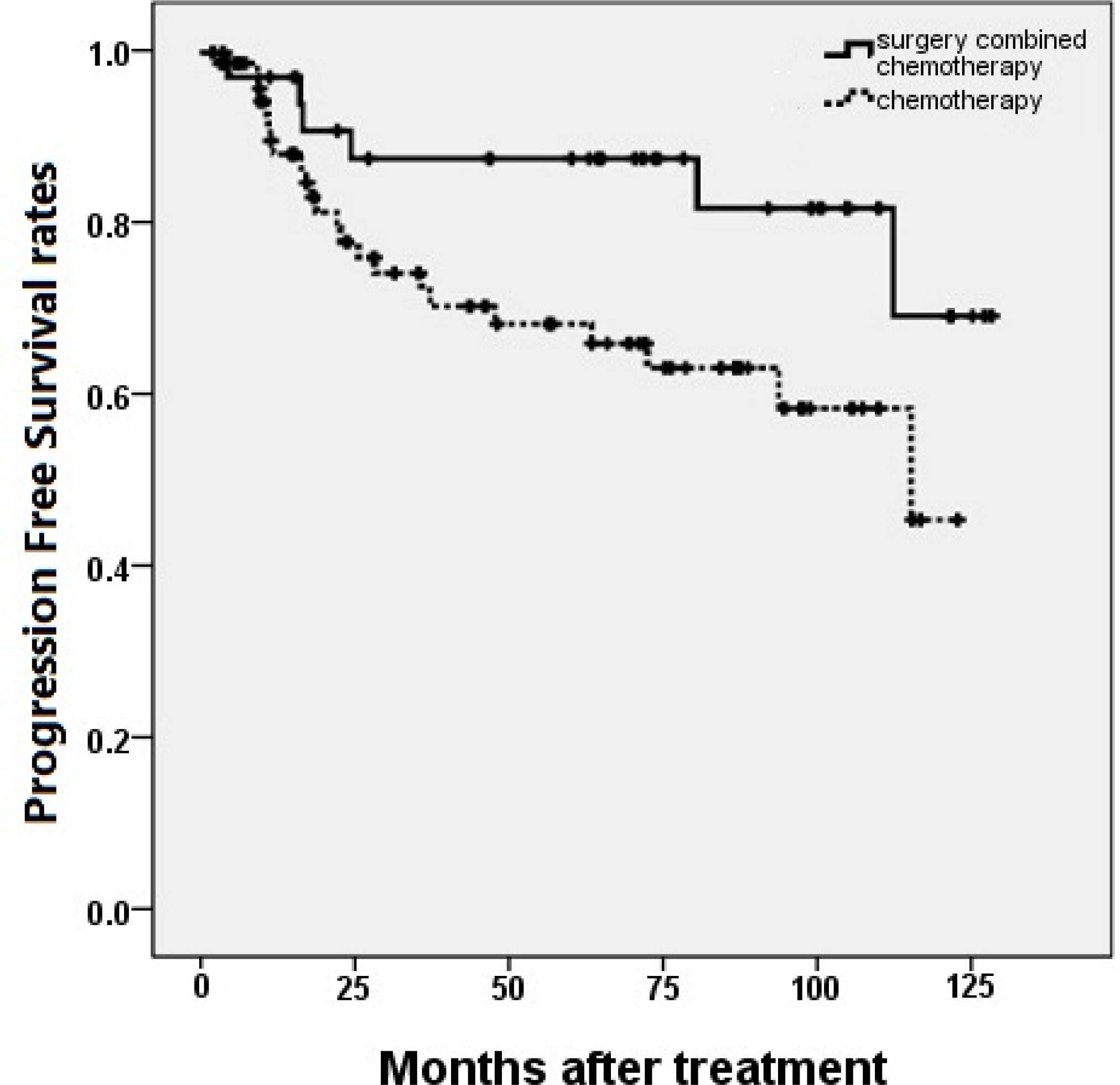
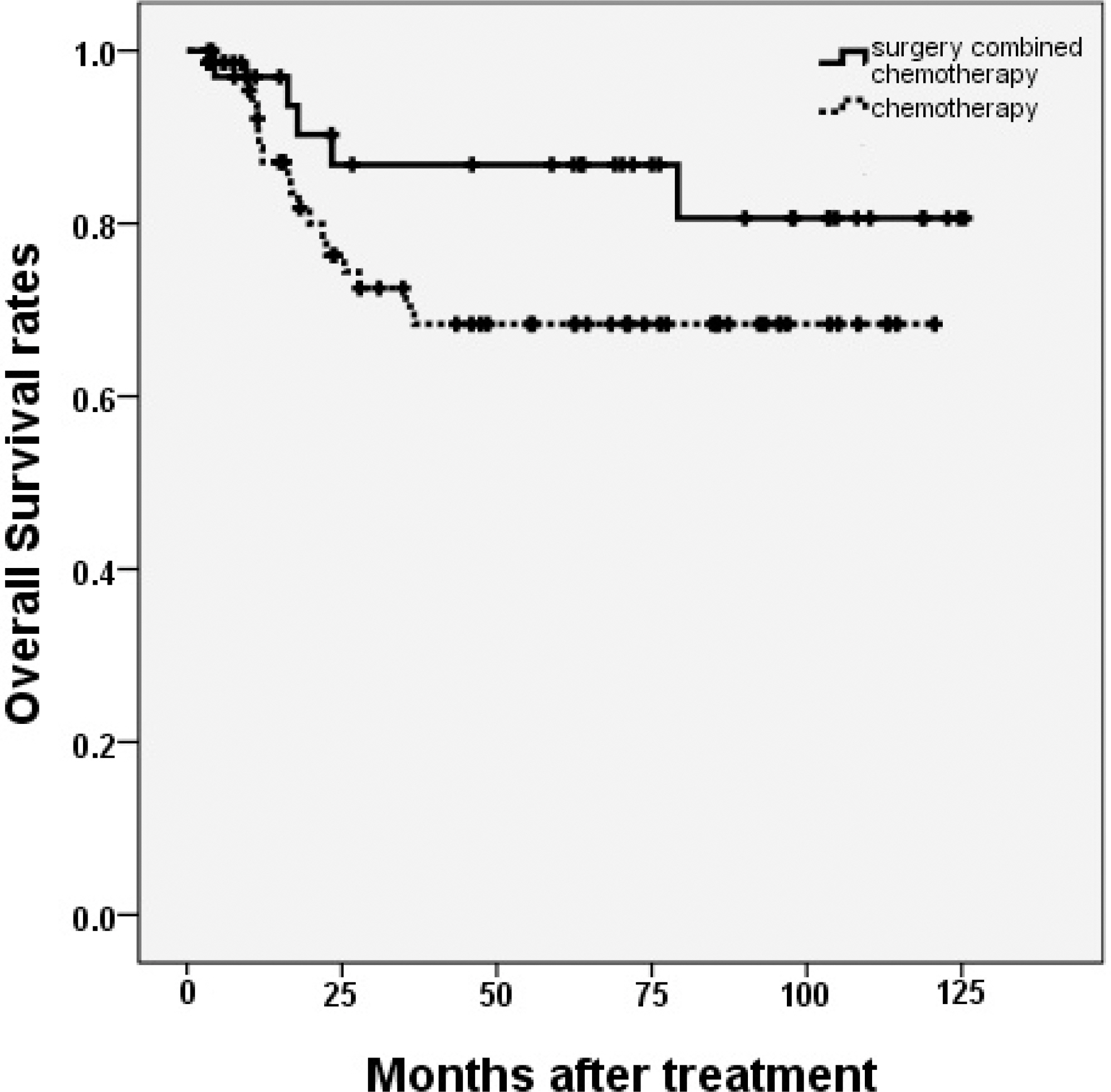
- The 5-year progression free survival rates (PFS) of group A and B were 86.7% and 66.1%, respectively (P = 0.037), while the 5-year overall survival rates (OS) were 86.8% and 68.4%, respectively (P = 0.129). In multivariate analysis, Both PFS and OS were not changed by treatment strategies (surgery combined with chemotherapy or chemotherapy only). The international prognostic index (IPI) was the only independent predictive factor for PFS.
-
Conclusions
- In our study, surgery combined with chemotherapy and chemotherapy only make no difference of survival rate. And further randomized prospective studies are needed to confirm a treatment strategies at improving survival outcomes in PGIL patients.
Figure 1.Progression free survival rates compared in patients according to the treatment strategy. Patients treated with surgery combined with chemotherapy were shown had superior 5-year progression free survival rates than chemotherapy only in patients with primary gastrointestinal lymphoma. (P = 0.037)
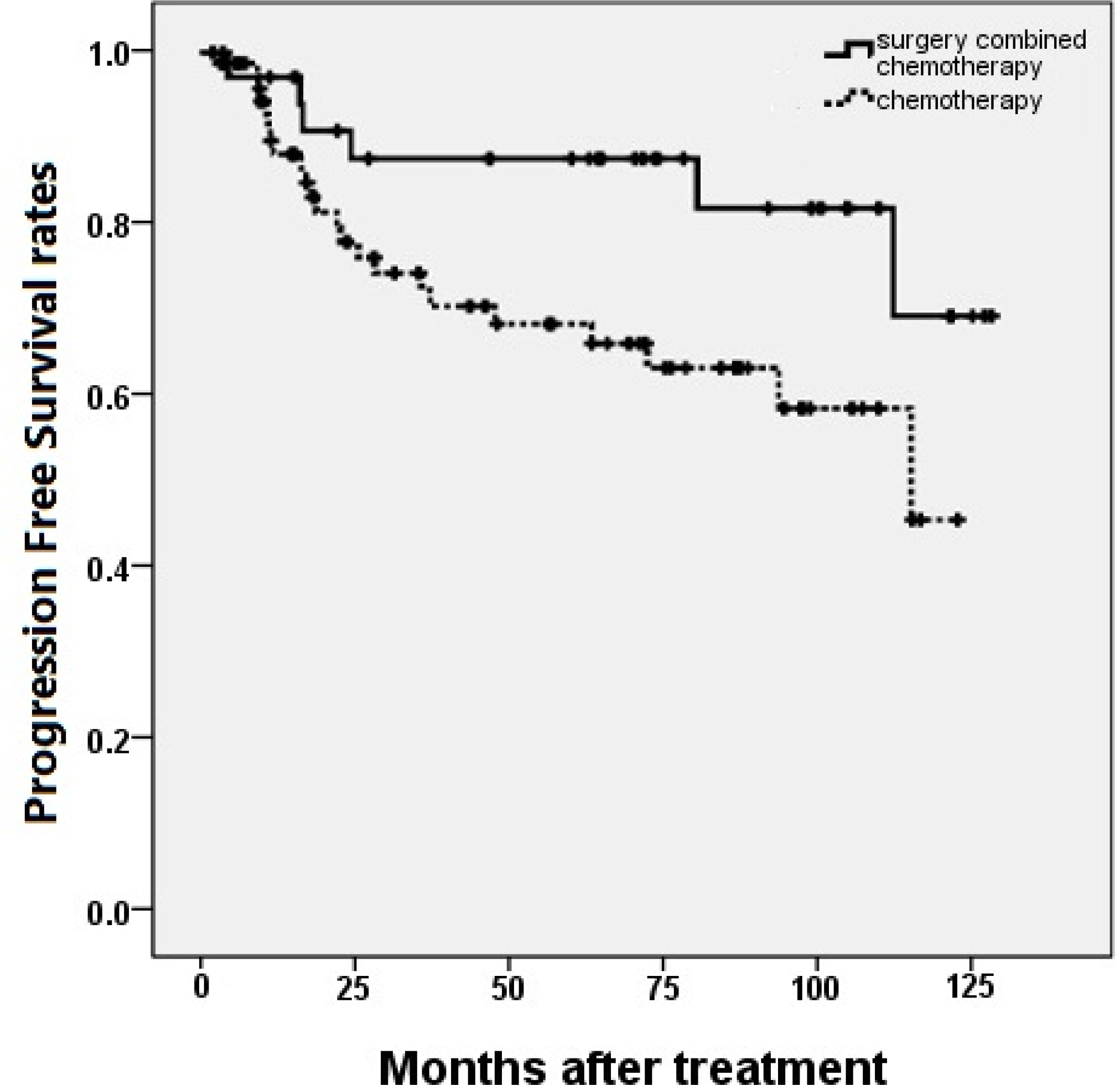
Figure 2.Overall survival rates compared in patients according to the treatment strategy. There was no significant difference in 5-year overall survival rates between patients with primary gastrointestinal lymphoma treated with surgery combined with chemotherapy and chemotherapy only in patients with primary gastrointestinal lymphoma. (P = 0.129)
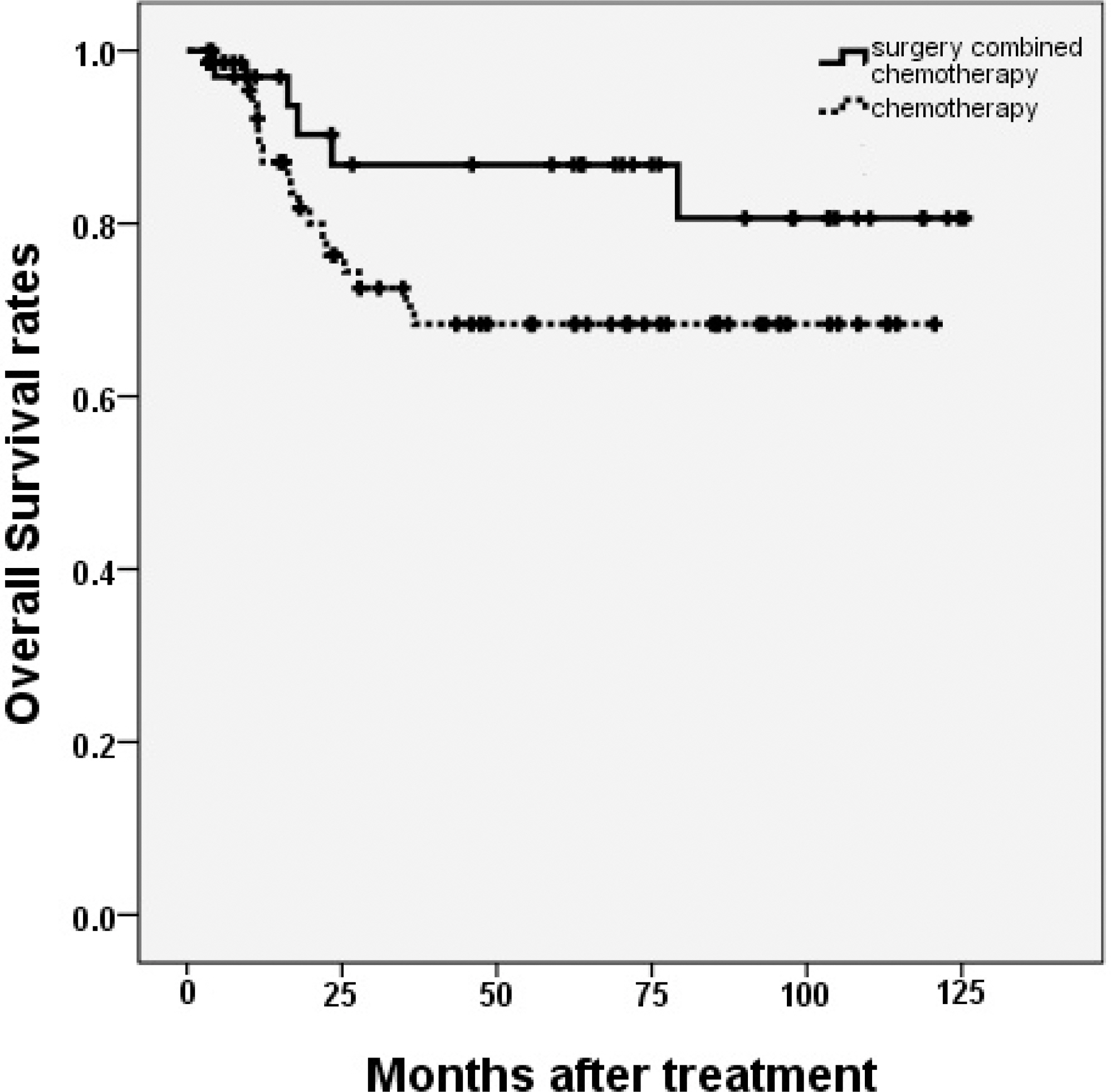
Table 1.The classification of PGIL according to Ann-Arbor staging system
Table 2Patient characteristics (N=107)
Table 3Comparison of patients based on a treatment strategy
Table 4Univariate analysis of prognostic factors
Table 5.Multivariate analysis of prognostic factors
- 1. LEE YJ, Lee JH. Gastrointestinal lymphoma, Korean J Helicobacter Up Gastrointest Res 2012;12:158–65.
- 2. d'Amore F, Brincker H, Gr⊘nbaek K, Thorling K, Pedersen M, Jensen MK, et al. Non-Hodgkin's lymphoma of the gastrointestinal tract: a population-based analysis of incidence, geographic distribution, clinicopathologic presentation features, and prognosis. Danish Lymphoma Study Group, J Clin Oncol 1994;12:1673–84.
- 3. Koch P, del Valle F, Berdel WE, Willich NA, Reers B, Hiddemann W, et al. Primary gastrointestinal non-Hodgkin's lymphoma: I. Anatomic and histologic distribution, clinical features, and survival data of 371 patients registered in the German Multicenter Study, J Clin Oncol 2001;19:3861–73.
- 4. Psyrri A, Papageorgiou S, Economopoulos T. Primary extranodal lymphomas of stomach: clinical presentation, diagnostic pitfalls and management, Ann Oncol 2008;19:1992–9.
- 5. Kim JM, Ko YH, Lee SS, Huh J, Kang CS, Kim CW, et al. WHO classification of malignant lymphomas in Korea: report of the third nationwide study, Korean J Pathol 2011;45:254–60.
- 6. Wündisch T, Thiede C, Morgner A, Dempfle A, Günther A, Liu H, et al. Long-term follow-up of gastric MALT lymphoma after Helicobacter pylori eradication. J Clin Oncol 2005;23:8018–24.ArticlePubMed
- 7. Wündisch T, Mösch C, Neubauer A, Stolte M. Helicobacter pylori eradication in gastric mucosa-associated lymphoid tissue lymphoma: Results of a 196-patient series, Leuk Lymphoma 2006;47:2110–4.
- 8. Koch P, Probst A, Berdel WE, Willich NA, Reinartz G, Brockmann J, et al. Treatment Results in Localized Primary Gastric Lymphoma: Data of Patients Registered Within the German Multicenter Study(GIT NHL 02/96). J Clin Oncol 2005;23:7050–9.ArticlePubMed
- 9. Binn M, Ruskone-Fourmestraux A, Lepage E, Haio-un C, Delmer A. Surgical resection plus chemotherapy versus chemotherapy alone: comparison of two strategies to treat diffuse large B-cell gastric lymphoma. Ann Oncol 2003;14:1751–7.ArticlePubMed
- 10. Jezers ek Novakovic B, Vovk M, Juznicsetina T. A single-center study of treatment outcomes and survival in patients with primary gastric lymphomas between 1990 and 2003. Ann Hematol 2006;85:849–56.ArticlePubMed
- 11. Avilés A, Nambo MJ, Neri N, Talavera A, Cleto S. Mucosa-associated lymphoid tissue (MALT) lymphoma of the stomach: results of a controlled clinical trial. Med Oncol 2005;22:57–62.ArticlePubMed
- 12. Medina-Franco H, Germes SS, Maldonado CL. Prognostic factors in primary gastric lymphoma, Ann Surg Oncol 2007;14:2239–45.
- 13. Kim SJ, Kang HJ, Kim JS, Oh SY, Choi CW, Lee SI, et al. Comparison of treatment strategies for patients with intestinal diffuse large B-cell lymphoma: surgical resection followed by chemotherapy versus chemotherapy alone. Blood 2011;117:1958–65.ArticlePubMed
- 14. Cirocchi R, Farinella E, Trastulli S, Cavaliere D, Covarelli P, Listorti C, et al, Surgical treatment of primary gastrointestinal lymphoma. World J Surg Oncol 2011;9:145.PubMedPMC
- 15. Lee J, Kim WS, Kim K, Ahn JS, Jung CW, Lim HY, et al. Prospective clinical study of surgical resection followed by CHOP in localized intestinal diffuse large B cell lymphoma. Leuk Res 2007;31:359–64.ArticlePubMed
- 16. Zinzani PL, Magagnoli M, Pagliani G, Bendandi M, Gherlinzoni F, Merla E, et al. Primary intestinal lymphoma: clinical and therapeutic features of 32 patients. Haematologica 1997;82:305–8.PubMed
- 17. Cheung MC, Housri N, Ogilvie MP, Sola JE, Koniaris LG. Surgery does not adversely affect survival in primary gastrointestinal lymphoma. J Surg Oncol 2009;100:59–64.ArticlePubMed
- 18. Beaton C, Davies M, Beynon J. The management of primary small bowel and colon lymphoma―a review. Int J Colorectal Dis 2012;27:555–63.ArticlePubMed
- 19. Lee J, Kim WS, Kim K, Ko YH, Kim JJ, Kim YH, et al. Intestinal lymphoma: exploration of the prognostic factors and the optimal treatment. Leuk Lymphoma 2004;45:339–44.ArticlePubMed
- 20. Daum S, Ullrich R, Heise W, Dederke B, Foss HD, Stein H, et al. Intestinal non-Hodgkin's lymphoma: a multicenter prospective clinical study from the German Study Group on Intestinal non-Hodgkin's Lymphoma. J Clin Oncol 2003;21:2740–6.ArticlePubMed
- 21. Azab MB, Henry-Amar M, Rougier P, Bognel C, Theodore C, Carde P, et al. Prognostic factors in primary gastrointestinal non-Hodgkin's lymphoma. A multivariate analysis, report of 106 cases, and review of the literature. Cancer 1989;64:1208–17.ArticlePubMed
- 22. Gou HF, Zang J, Jiang M, Yang Y, Cao D, Chen XC. Clinical prognostic analysis of 116 patients with primary intestinal non-Hodgkin lymphoma. Med Oncol 2012;29:227–34.ArticlePubMed
References
Figure & Data
References
Citations
Citations to this article as recorded by 
 PubReader
PubReader ePub Link
ePub Link Cite
Cite