 KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Volume 30(2); 2015 > Article
-
Original Article
Complications caused by perfluorocarbon liquid used in pars plana vitrectomy - Jae Ho Yoo1, Ki Yup Nam2, Seung Uk Lee2, Ji Eun Lee2, Sang Joon Lee2
-
Kosin Medical Journal 2015;30(2):123-130.
DOI: https://doi.org/10.7180/kmj.2015.30.2.123
Published online: January 20, 2015
1Oksan Health Subcenter, Euiseong-Gun, Korea
2Department of Ophthalmology, College of Medicine, Kosin University, Busan, Korea
- Corresponding Author: Sang Joon Lee, Department of Ophthalmology, College of Medicine, Kosin University, 262, Gamcheon-ro Seo-gu, Busan 49267, Korea TEL: +82-51-990-6228 FAX: +82-51-990-3026 E-mail: hhiatus@gmail.com
• Received: February 20, 2014 • Accepted: July 9, 2014
Copyright © 2015 Kosin University School of Medicine Proceedings
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,324 Views
- 8 Download
- 1 Crossref
Abstract
-
Objectives
- To assess the inadvertent intraocular retention of perfluorocarbon liquid (PFCL) after vitreoretinal surgery and their complications.
-
Methods
- We retrospectively reviewed the medical records of 108 patients who underwent vitreoretinal surgeries using intraoperative PFCL (perfluoro-n-octane (C8F18), 0.69 centistoke at 25℃, PERFLUORN®, Alcon, USA) and the removal of PFCL through fluid-air exchange. The analysis was focused on the occurrence of intraocular retained PFCL, diagnoses, surgicalprocedures, and complications.
-
Results
- Retinal detachment (51 cases, 47%) was the most common surgery which used PFCL intraoperatively. Other causes were vitreous hemorrhage (24 cases, 22%), posteriorly dislocated lens (22 cases, 21%), and trauma (11 cases, 10%). Intraocular PFCL was found in a total of 9 (8.3%) eyes. PFCL bubbles remained in anterior chamber and vitreous cavity were observed in 4 cases and subretinal retained PFCL was observed in 5 cases. Three of 5 cases of subretinal PFCL exhibited in subfoveal space. Among the three subfoveal cases, macular hole developed after PFCL removal in 1 case, epiretinal membrane in the area where had been PFCL bubble. However, we observed no complications in 1 case of subfoveal PFCL that was removed by surgery. PFCL in anterior chamber and vitreous cavity were in 4 cases.
-
Conclusions
- The presence of subfoveal PFCL might affect visual and anatomic outcomes. However, subfoveal PFCL may induce visual complications, and therefore requires special attention.
Fig. 1.A. Anterior segment Photo shows multiple PFCL bubble in inferior anterior chamber.(red arrow) B. Postoperative retinography of case 5 showing multiple PFCL spheres in the posterior pole, extramacular.(red arrow) After 2 years, notice the reflexes caused by PFCL. The patient's visual acuity was 0.25. C. Postoperative retinography shows PFCL bubble at superior side of macula.(red arrow) D.Vertical OCT section of the "C" case was shown and the intraretinal black hollow (arrow head) was PFCL subretinal bubble.
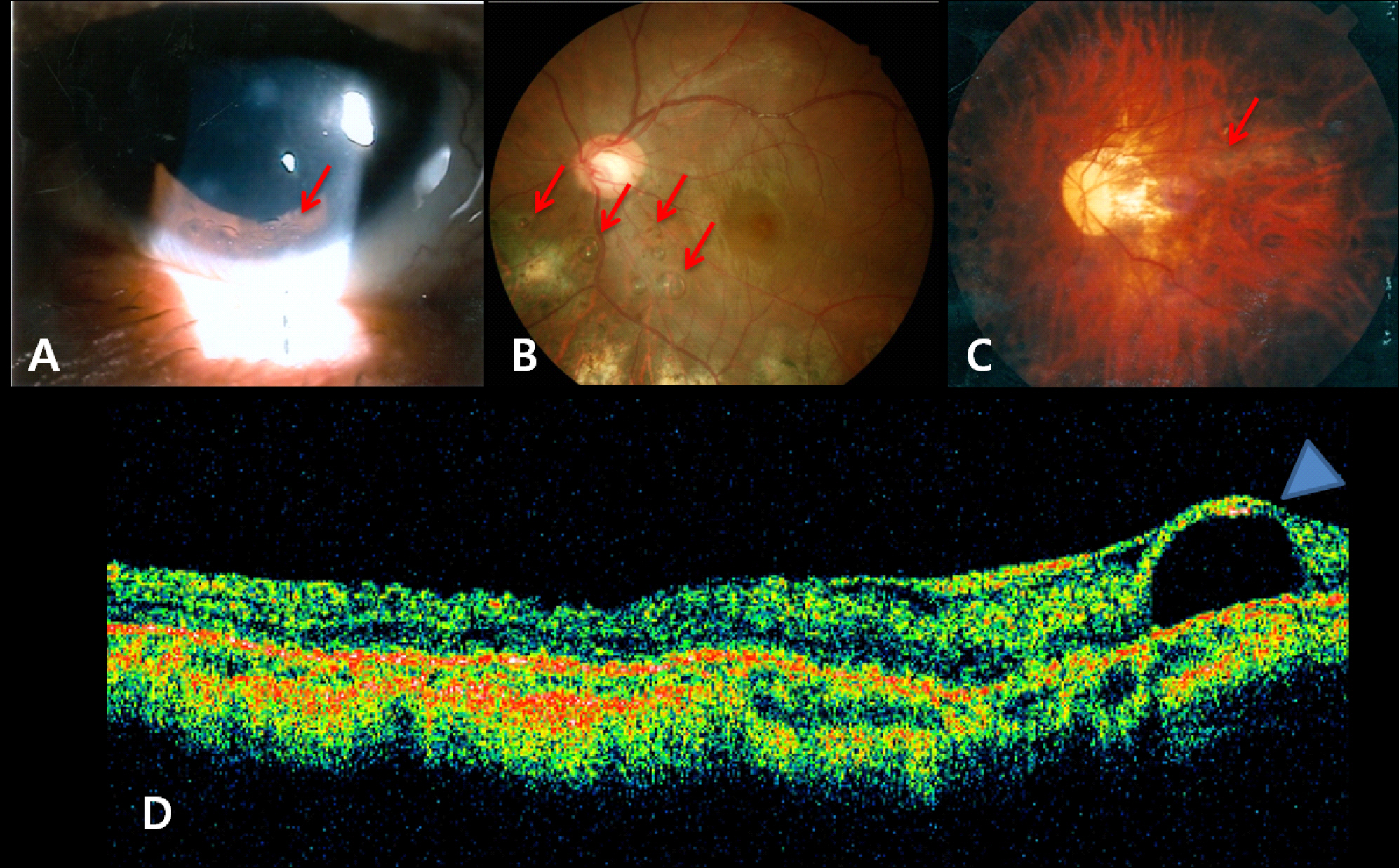
Fig 2.A. Retinography shows round reflex at macular due to subfoveal PFCL and atrophic change around posterior pole due to laser treatment. B. After 48 months with secondary IOL implant, retinography shows no obvious anatomy changes.(red arrow) The patients last visual acuity was 0.125. C.Vertical OCT section of the "B" case was shown and subfoveal PFCL bubble was observed.(blue arrow head) D. Postoperative retinography showing yellowish glistening macula due to submacular PFCL.(red arrow) E. After 6 months, retinography shows inferiorly displaced PFCL (red arrow) and premacular gliosis and epiretinal membrane.(blue arrow head)
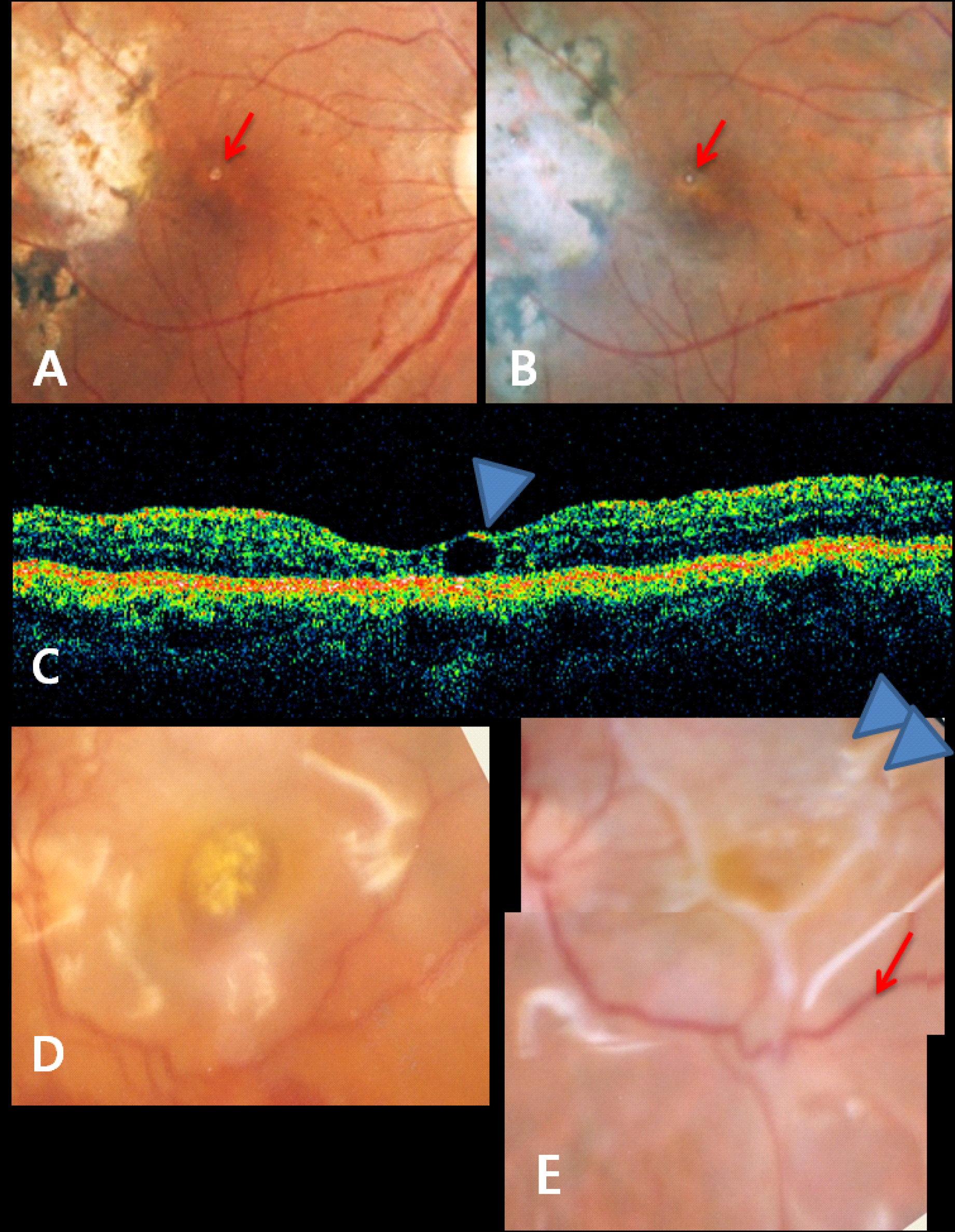
Table 1.Demographics of total patient and retained PFCL cases.
Table 2.Cumulative Percent of Eyes with Retained Perfluorocarbon Liquid
Table3.Patient Characteristics with retained PFCL
- 1. Lesnoni G, Rossi T, Gelso A. Subfoveal liquid perfluorocarbon. Retina 2004;24:172–6.ArticlePubMed
- 2. Chang S, Lincoff H, Zimmerman NJ, Fuchs W. Giant retinal tears. Surgical techniques and results using perfluorocarbon liquids. Arch Ophthalmol 1989;107:761–6.ArticlePubMed
- 3. Peyman GA, Schulman JA, Sullivan B. Perfluorocarbon liquids in ophthalmology. Surv Ophthalmol 1995;39:375–95.ArticlePubMed
- 4. Han DP, Nanda SK, O'Brien WJ, Guy J, Murray TG, Boldt HC. Evaluation of anterior segment tolerance to short-term intravitreal perfluoron. Retina 1994;14:219–24.ArticlePubMed
- 5. Tanji TM, Peyman GA, Mehta NJ, Millsap CM. Perfluoroperhydrophenanthrene (Vitreon) as a short-term vitreous substitute after complex vitreoretinal surgery. Ophthalmic surgery 1993;24:681–5.ArticlePubMed
- 6. Garcia-Valenzuela E, Ito Y, Abrams GW. Risk factors for retention of subretinal perfluorocarbon liquid in vitreoretinal surgery. Retina 2004;24:746–52.ArticlePubMed
- 7. Bourke RD, Simpson RN, Cooling RJ, Sparrow JR. The stability of perfluoro-N-octane during vitreoretinal procedures. Archives of ophthalmology 1996;114:537–44.ArticlePubMed
- 8. Scott IU, Murray TG, Flynn HW, Jr. , Smiddy WE, Feuer WJ, Schiffman JC. Outcomes and complications associated with perfluoro-n-octane and perfluoroperhydrophenanthrene in complex retinal detachment repair. Ophthalmology 2000;107:860–5.ArticlePubMed
- 9. Viebahn M, Buettner H. Perfluorophenanthrene unsuitable for postoperative retinal tamponade. Am J Ophthalmol 1994;118:124–6.ArticlePubMed
- 10. Moreira H, de Queiroz JM, Jr. , Liggett PE, McDonnell PJ. Corneal toxicity study of two perfluorocarbon liquids in rabbit eyes. Cornea 1992;11:376–9.ArticlePubMed
- 11. Alster Y, Ben-Nun Y, Loewenstein A, Lazar M. Pupillary block glaucoma due to residual perfluorodecalin. Ophthalmic Surg Lasers 1996;27:395–6.ArticlePubMed
- 12. Aydin E, Demir HD. Perfluorodecaline residue in the anterior chamber of a patient with an intact crystalline lens: a case report. J Med Case Rep 2008;2:13.ArticlePubMedPMC
- 13. Wilbanks GA, Apel AJ, Jolly SS, Devenyi RG, Rootman DS. Perfluorodecalin corneal toxicity: five case reports. Cornea 1996;15:329–34.ArticlePubMed
- 14. Rofail M, Lee LR. Perfluoro-n-octane as a postoperative vitreoretinal tamponade in the management of giant retinal tears. Retina 2005;25:897–901.ArticlePubMed
- 15. Eckardt C, Nicolai U, Winter M, Knop E. Experimental intraocular tolerance to liquid perfluorooctane and perfluoropolyether. Retina 1991;11:375–84.ArticlePubMed
- 16. Vilaplana D, Poposki V, Martinez-Palmer A, Castilla M. [Subfoveal perfluorocarbon liquid. Two new cases]. Arch Soc Esp Oftalmol 2009;84:363–6.PubMed
- 17. Escalada Gutierrez F, Mateo Garcia C. [Extraction of subfoveal liquid perfluorocarbon]. Arch Soc Esp Oftalmol 2002;77:519–21.PubMed
- 18. Wong TY, Ho T. Retained perfluorodecalin after retinal detachment surgery. Int Ophthalmol 1996;20:293–4.ArticlePubMed
References
Figure & Data
References
Citations
Citations to this article as recorded by 
- Trocar blade-assisted skewer technique for phacoemulsification of a dislocated lens
Laura Liu, Yih-Shiou Hwang, Wei-Chi Wu, Chi-Chun Lai, Jorn-Hon Liu
Taiwan Journal of Ophthalmology.2024; 14(1): 129. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite

